UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
☑ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES
EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2015
¨ TRANSITION REPORT UNDER SECTION 13 OR 15(d) OF THE SECURITIES
EXCHANGE ACT OF 1934
Commission file number 000-52534

PARALLAX HEALTH SCIENCES, INC.
(Exact name of registrant as specified in its charter)
Nevada | 46-4733512 |
(State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) |
|
|
1327 Ocean Avenue, Suite B, Santa Monica, CA | 90401 |
(Address of principal executive offices) | (Zip Code) |
|
|
Registrant's telephone number, including area code: | (310) 899-4442 |
Copy of all Communications to:
Lawrence I. Washor
Washor & Associates
21800 Oxnard Street, Suite 790
Woodland Hills, CA 91367
(310) 479-2660
|
| |||||
|
| |||||
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 the Securities Act. | Yes ¨ No ☑ | |||||
|
| |||||
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. | Yes ¨ No ☑ | |||||
|
| |||||
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports) and (2) has been subject to such filing requirements for the last 90 days. | Yes ¨ No ☑ | |||||
|
| |||||
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registration statement was required to submit and post such files). | Yes ¨ No ☑ | |||||
|
| |||||
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. | Yes ¨ No ☑ | |||||
| ||||||
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definition of "large accelerated filer," "accelerated filer" and "smaller reporting company" in Rule 12b-2 of the Exchange Act. | ||||||
| ||||||
| Large accelerated filer | ¨ |
| Accelerated filer | ¨ |
|
| Non-accelerated filer | ¨ |
| Smaller reporting company | ☑ |
|
| ||||||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). | Yes ¨ No ☑ | |||||
|
| |||||
|
| |||||
The aggregate market value of Common Stock held by non-affiliates of the Registrant as of June 30, 2015 was $1,367,647, based on a closing price of $0.062 for the Common Stock on June 30, 2015, the last business day of the Registrant's most recently completed second fiscal quarter. For purposes of this computation, all executive officers and directors have been deemed to be affiliates. Such determination should not be deemed to be an admission that such executive officers and directors are, in fact, affiliates of the Registrant.
Indicate the number of shares outstanding of each of the registrant's
classes of common stock as of the latest practicable date.
111,532,620 Common Shares issued and outstanding as of June 15, 2017
TABLE OF CONTENTS | ||
| ||
ITEM 1. | BUSINESS | 3 |
|
|
|
ITEM 1A. | RISK FACTORS | 24 |
|
|
|
IT E M 2. | PROPERTIES | 2 4 |
|
|
|
ITEM 3. | LEGAL PROCE EDINGS | 24 |
|
|
|
ITEM 4. | MINE SAFETY STANDARDS | 24 |
|
|
|
ITEM 5. | MARKET FOR COMMON EQUITY AND RELATED STOCK HOLDER MATTERS | 25 |
|
|
|
ITEM 6. | SELECTED FINANCIAL DATA | 27 |
|
|
|
I TE M 7. | MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS | 27 |
|
|
|
ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOU T MARKET RISKS | 32 |
|
|
|
ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA | 32 |
|
|
|
ITEM 9. | CHANGES IN AND DISAGREEMEN TS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE | 33 |
|
|
|
ITEM 9A. | CO NTROLS AND PROCEDURES | 33 |
|
|
|
ITEM 9B. | OTHER INFOR MATION | 34 |
|
|
|
ITEM 10. | DIRECTORS, EXE CUTIVE OFFICERS AND CORPORATE GOVERNANCE | 34 |
|
|
|
ITE M 11. | EXECUTIVE COMPENSATION | 40 |
|
|
|
ITE M 1 2. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS | 41 |
|
|
|
ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE | 42 |
|
|
|
ITEM 14. | PRINCIPAL ACCOUNTANTS FEES AND SERVICES | 43 |
|
|
|
ITEM 15. | EXHIBITS, FINANCIAL STATEMENT SCHEDULES | 44 |
2
PART I
ITEM 1. | BUSINESS |
As used in this annual report, the terms "we", "us", "our" and "Parallax" mean Parallax Health Sciences, Inc. (the "Company"), and its wholly-owned subsidiaries, Parallax Diagnostics, Inc. (formerly Endeavor Sciences, Inc.) and RoxSan Pharmacy, Inc., unless otherwise indicated.
This annual report contains forward-looking statements. These statements relate to future events or the Company's future financial performance, and include statements made by the Company regarding product development and obtaining FDA clearances. In some cases, forward-looking statements can be identified by terminology such as "may", "should", "expects", "plans", "anticipates", "believes", "estimates", "predicts", "potential" or "continue" or negative of these terms or other comparable terminology. These statements are only predictions and involve known and unknown risks, uncertainties and other factors" that may cause the Company's or its industry's actual results, levels of activity, performance or achievements to be materially different from any future results, levels of activity, performance or achievements expressed or implied by these forward-looking statements.
Although the Company believes that the expectations reflected in the forward-looking statements are reasonable, it cannot guarantee future results, levels of activity, performance or achievements. Except as required by applicable law, including the securities laws of the United States, the Company does not intend to update any of the forward-looking statements to conform these statements to actual results.
The Company's financial statements are stated in United States Dollars (US$) and are prepared in accordance with United States Generally Accepted Accounting Principles.
In this annual report, unless otherwise specified, all dollar amounts are expressed in United States Dollars and all references to "common shares" refer to the common shares in the Company's capital stock.
CORPORATE OVERVIEW
The Company's principal executive office is located at 1327 Ocean Avenue, Suite M, Santa Monica, California, 90401, with operations at 465 N. Roxbury Drive, Beverly Hills, CA 90210. The Company's telephone numbers are (310) 899-4442 (Santa Monica) and (310) 273-1644 (Beverly Hills).
The Company's websites are at www.paralla xhealthsciences.com , www.parallaxdiagnostics.com , www.roxsan.com and www.roxsanfertility.com
The Company is a fully reporting company with its stock traded on the OTC Markets under the symbol "PRLX".
Corporate History
Formation and Development
The Company was incorporated in the State of Nevada on July 6, 2005. On November 1, 2012, the Company, formerly Endeavor Power Corporation, and its wholly owned subsidiary Endeavor Holdings, Inc., a Nevada corporation, entered into an Agreement and Plan of Merger with Parallax Diagnostics, Inc., a Nevada corporation ("Parallax Diagnostics" or "PDI"), whereby Parallax Diagnostics became a wholly owned subsidiary. On January 9, 2014, the Company changed its name to Parallax Health Sciences, Inc. ("Parallax"). (OTC.PRLX).
Parallax Diagnostics was founded in 2010, and holds the right, title, and interest in perpetuity to certain Target System Immunoassay point-of-care diagnostic testing system and related FDA-cleared tests in the area of infectious disease. Its primary focus was to commercialize the proprietary testing system and test in a worldwide domain.
Parallax Diagnostics is currently pre-revenue, and continues to pursue viable opportunities for the commercialization of its product. The Company has sought to identify strategies that would make its proposition more valuable and competitive. To this end, the Company has pursued the creation of patents around its foundational technology, and began developing a novel immune status test targeting the HIV/AIDS and TB markets. Since the inception of Parallax Diagnostics, and the Company has been issued patents on elements of its technology for its testing system.
In 2013, Parallax identified an opportunity to acquire RoxSan Pharmacy, Inc. ("RoxSan"), a California corporation, and began the due diligence process. The Company's initial interest centered on utilizing the acquisition as a means of accelerating the commercialization of the Parallax Target System and diagnostic platform, as RoxSan had access to a nationwide network of doctors and sales representatives. During the due diligence process, the Company became aware of the numerous opportunities that RoxSan and its markets represented.
On March 21, 2013, the Company entered into a Letter of Intent with Shahla Melamed, RoxSan's sole Shareholder, to acquire RoxSan. Between 2013 and 2015, four (4) amendments were also executed.
Table of Contents
3
As part of the acquisition, the Company was required to obtain licensure from the State of California, and on July 31, 2015, the Company received notice that its pharmacy and sterile compounding licenses were issued by the California State Board of Pharmacy.
On August 13, 2015 (the "Closing Date"), pursuant to a resolution of the board of directors (the "Board"), the Company entered into an Agreement to Purchase and Sell One Hundred Percent of the Issued and Outstanding Shares of RoxSan Pharmacy, Inc. ("RoxSan" or the "Pharmacy"), and its Assets and Inventory (the "Purchase Agreement"). Pursuant to the Purchase Agreement between the Company, RoxSan and its sole shareholder, Shahla Melamed (the "Seller" or "Melamed"), in exchange for 100% of RoxSan's common stock, and its assets and inventory, the Company, among other things, issued the Seller a Secured Promissory Note (the "Note") dated August 13, 2015 in the amount of $20.5 million (the "Acquisition"). The Note bears interest at a rate of 6% per annum, and matures in three (3) years, or August 13, 2018 ("Maturity"). Principal and interest payments on the Note will be made to the Seller on a quarterly basis beginning with the three-month period ending November 30, 2015, in an amount equal to: 1) 75% during the first two (2) years; and 2) 60% during year three (3); of certain of the Pharmacy's earnings defined within the Purchase Agreement as EBITDA. All remaining principal and/or accrued interest, if any, still owing after three (3) years shall be paid in full to the Seller at Maturity. The Company is seeking a reduction in the Purchase Price and related promissory note (See Legal Proceedings).
As a result of the Acquisition, effective August 13, 2015, RoxSan became a wholly owned subsidiary of the Company. No change in control of the Company occurred as a result of the Acquisition.
In connection with the Acquisition, the Company entered into an Employment Agreement (the "Employment Agreement") with the Seller. Under the Employment Agreement, Melamed agreed to provide exclusive consulting services to the Company in the areas of public relations and marketing for a term of four (4) years. On March 4, 2016, the Company terminated the Employment Agreement in accordance with paragraph 3.2 Termination for Cause (see "Dispute with Former Owner" below). The termination was the result of, among other things, Melamed's breaches in the Agreement, which were substantiated by an investigation conducted by an employment law firm retained by RoxSan. Under the terms of the Agreement, no financial obligation resulted in the termination.
On October 15, 2015, Mr. Edward W. Withrow III resigned as chairman and member of the Board. This resignation did not involve any disagreement with the Company. Prior to the submission of his resignation, Mr. Withrow asked Mr. David M. Engert, an existing board member, to succeed him as Executive Chairman. Mr. Engert accepted the position, under the condition that he receive a Consulting Agreement wherein he would receive compensation at a rate of $180,000 per annum in exchange for a part-time commitment. Pursuant to the Consulting Agreement, Mr. Engert's duties were as follows:
1.
Oversee the governance and function of the Board
2.
Advise on capitalization matters and financing:
a.
Perform or review due diligence on capital source
b.
Introduce the Company to potential strategic partners
c.
Interface with NASDAQ or AMEX executives as part of the Company's up-listing goals
d.
Develop capitalization materials and interface with the financial community
3.
Advise on Merger & Acquisition (M&A) opportunities:
a.
Assist in the development of acquisition strategies
b.
Interface with outside M&A professionals,
c.
Interface with executives, boards and/or control investors of companies that represent potential targets for acquisition.
In addition, as part of Mr. Engert's Consulting Agreement, the Company was obligated to pay for Mr. Engert's travel to the Company's headquarters in California, as Mr. Engert resides in Arizona.
Over time, management became aware that Mr. Engert, aside from the duties he was retained to perform, began to involve himself with the management, oversight and strategic planning of the business of RoxSan. This resulted in, among other things, a substantial amount of managerial overlapping and duplication. As a result, during the first quarter of 2016, the Company's President notified Mr. Engert that, as his services were not physically required at RoxSan, and in an effort to be financially prudent, he would no longer need to travel to the Company's offices.
Management reiterated several times to Mr. Engert the Company's need for the services that he was hired to perform, outside of his role as Executive Chairman. Mr. Engert stated that he was not inclined to perform the functions around securing capital, investment banking introductions and other services, for various reasons.
During the 4th quarter 2016, members of the Company's management team, members of the Board and Mr. Engert were involved in a disagreement over certain content included in a Consent Resolution presented to the Board for approval (the "Resolution"). Though the content was ultimately removed from the Resolution, Mr. Engert was at odds with the Board over the Resolution's content, as well as the participation and role of the Company's Majority Shareholders with regards to the Board and its deliberations.
On December 29, 2016, in accordance with the Company's by-laws, a meeting of shareholders representing over fifty percent (50%) of the Company's issued and outstanding shares, was held, wherein a vote was taken to elect and re-elect the Company's Board members. During this meeting, Mr. Engert was not re-elected.
4
As a result of the disagreement with Mr. Engert, he has filed a lawsuit in Arizona claiming, among other issues, monies owed to him under his Consulting Agreement for being terminated without cause. The Company is in disagreement with the position and claims made by Mr. Engert, and as such have notified Mr. Engert that the Company intends to vigorously defend its position. Management believes a good faith attempt at resolving this matter outside of the courthouse is in the best interest of the Company and its shareholders.
During the shareholders meeting held on December 29, 2016, Mr. John L. Ogden and Ms. Calli R. Bucci were elected to serve as members of the Company's board of directors. On April 6, 2017, the Board elected Mr. Joseph M. Redmond as Chairman, to serve until the Company's next meeting, in accordance with the Company's bylaws, or a resignation is duly tendered.
Effective July 7, 2017, the Board of the Company has caused the departure of Mr. Redmond from his position as President and Chief Executive Officer of the Company. Pursuant to the Employment Agreement dated August 1, 2015, Mr. Redmond resigned from the Board of the Company and its wholly-owned subsidiary, RoxSan Pharmacy, Inc.
Effective July 7, 2017, pursuant to a unanimous Board resolution, Mr. Paul R. Arena was appointed as the Company's President and Chief Executive Officer, and the Board caused Mr. Arena's election to the Company's Board and the Board of its wholly-owned subsidiary, RoxSan Pharmacy, Inc.
In connection with Mr. Arena's appointment, the Company entered into an Executive Employment Agreement (the "Agreement") with Mr. Arena dated July 7, 2017, wherein Mr. Arena's will serve as President and Chief Executive Officer for a period of three (3) years. As compensation for his services, Mr. Arena will receive a base compensation of Three Hundred Fifty Thousand Dollars ($350,000) per annum in year one, of which 30% shall be deferred until certain funding goals are met; Four Hundred Twenty Five Thousand dollars ($425,000) in year two; and Five Hundred Fifty Thousand ($550,000) in year three.
Pursuant to the Agreement, Mr. Arena shall also be entitled to twice (2x) the base salary in any given year the Company's EBITDA reaches or exceeds the following: a) $1,000,000 generated by any individual division of the Company the first twelve month period following the date of the Agreement; b) $3,000,000 on a consolidated basis the second twelve month period; and c) $5,000,000 on a consolidated basis the third twelve month period. In the event the Company has not reached certain earnings/profits goals, Mr. Arena's base salary shall remain at the rate of Three Hundred Fifty Thousand Dollars ($350,000) per annum, or previous year, as the case may be, until the earnings/profits goals have been reached.
In connection with the Agreement, the Company has agreed to cause the issuance of ten million (10,000,000) shares of restricted common stock to Mr. Arena, of which 25% vests immediately upon execution of the Agreement; 25% vests one year from the date of the Agreement; 25% vests after two years from the date of the Agreement; and 25% vests when certain funding goals have been met.
Also, in connection with the Agreement, Mr. Arena shall be granted five million (5,000,000) stock options at an exercise price of twenty five cents ($0.25) per share. The options are for a period of five years, and vest as follows: a) 25% immediately upon execution of the Agreement; b) 25% when the Company's stock trades above forty cents ($0.40) per share for a period of thirty (30) days; c) 25% when the Company's stock trades above seventy-five cents ($0.75) per share for a period of sixty (60) days; and d) 25% when the Company's stock trades at over one dollar ($1.00) per share for a period of ninety (90) days.
Dispute with Former Owner of Pharmacy
Shortly after the Closing, the Company's management and Melamed clashed over control of the RoxSan Pharmacy business operations and bank accounts. Faced with Melamed continuing to materially interfere with the Pharmacy's operations to the detriment of its business, the Company retained the services of an employment law firm to investigate Melamed's actions, and provide a report to the Company's Board (the "Report"). The Company also placed Melamed on a paid leave of absence because of her actions. The Board, after reviewing the findings in the Report, found substantive cause for Melamed's termination, and immediately sent Melamed written notification of the Company's intent to dismiss her for cause. Under the Employment Agreement, Melamed was provided with a thirty (30) day cure period. However, the Company received no response of intent to cure from Melamed or her counsel, and no evidence of a cure was provided to the Company. As a result, the Board authorized Melamed's termination for cause on March 3, 2016, and on March 6, 2016, Melamed was formally terminated in writing.
In the course of management's operation of the RoxSan Pharmacy, and adherence to Financial Accounting Standards Board revenue recognition policies, management became concerned with the absence of the claim processing for over $16 million of pre-Close Workers Compensation prescription revenues, which Melamed represented to the Company prior to Closing as being the vast majority of the high margin compound revenue. In addition to the $16 million in pre-Close claims, the Pharmacy generated over $8 million after the change in ownership, until the CFO alerted management of a serious and dramatic change in the receivables collection timetable, the underpinning cash flow processes, and the potential illegitimacy of the Workers Compensation revenues. Further, the CFO was uncomfortable with recognizing the revenue as it was presented by Melamed's financial records, and, in the absence of any reasonable assurance of collectability of the Workers Compensation revenues, the Company established an allowance for doubtful receivables for the $8 million in post-Close claims for which collectability was highly unlikely.
Table of Contents
5
The Company retained the services of a forensic Workers Compensation fraud specialist to determine the legitimacy of the pre-Close Workers Compensation revenues and related insurance claims. As a result of this forensic review, it was determined that these claims were essentially valueless . As a result of these findings and undisclosed changes to the cash flow and quality of earnings that represented a majority of the revenue of the Pharmacy, the Company's Board deemed it necessary to demand a reduction in the terms of the Sale and Purchase Agreement to more accurately reflect the true valuation of the Company. This was met with resistance on the part of the Seller.
Shortly thereafter, in October 2015, Melamed, initiated two (2) legal actions against the Company in the Superior Court of the State of California, County of Los Angeles, West District, Shahla Melamed v. Parallax Health Sciences, Inc., action numbers SC 124873 and SC 125705 (the "Matter"). In the Matter, action No. SC124873, Melamed sought rescission of the August 13, 2015 Purchase Agreement. Rescission was sought on the basis that, allegedly, in order to acquire the Pharmacy, the Company and its principals had allegedly defrauded Melamed, there had allegedly been a complete failure of consideration, and a unilateral mistake was allegedly made on the part of Melamed.
On March 17, 2017, the Court ruled in favor of the Company, and issued that Melamed is not entitled to rescission of the Purchase Agreement. The ruling of the Court stated that no fraud on the part of the Company or its principals had been demonstrated. The Court further ruled that there had been no failure of consideration, and that Melamed's entry into the Agreement was not a result of a unilateral mistake on the part of Melamed. The Minutes of the Ruling were entered by the County Clerk on March 17, 2017.
The Company has likewise initiated legal action against Melamed and filed an action in the Superior Court of the State of California, County of Los Angeles, West District, Parallax Health Sciences, et al. v. Shahla Melamed, et al., case number SC 124898. The Complaint in that action alleges that Melamed has breached several obligations under the Purchase Agreement, and the Company is seeking to reduce the Secured Note due to undisclosed material changes in the business.
Subsequently filed pleadings by the Company and RoxSan in case number SC 124873 allege, among other things, that Melamed misrepresented the true earnings and source of income for the pharmacy business and had engaged in a fraudulent and illegal scheme to ship medications to states where her pharmacy was not licensed prior to the sale of the Pharmacy.
In the Matter, action No. SC125702, Melamed alleges that the Company is in default under the terms of the Purchase Agreement and Secured Note and the Company's termination of Melamed's employment agreement. The Company firmly believes that it had adequate grounds to justify the termination of the employment, that it acted within its rights, and shall prevail in these proceedings.
All three (3) legal matters are currently pending.
Description of Business
The Company's principal focus is on personalized patient care through the Company's Pharmacy, RoxSan, and eventually through the diagnostic testing platform capable of diagnosing and monitoring several health issues. Through the Company's wholly owned subsidiary Parallax Diagnostics Inc., the Company holds the right, title, and interest in perpetuity to certain point-of-care diagnostic tests.
The Company has the following two business segments: Retail Pharmacy Services (RPS) and Corporate.
Retail Pharmacy Services (RPS)
The RPS provides a full range of pharmacy services including retail, compounding and fertility medications.
The RPS generates net revenues primarily by dispensing prescription drugs, both through local channels by direct delivery as well as mail order. The RPS also sells a wide assortment of general merchandise, including over-the-counter drugs, beauty products and cosmetics, seasonal merchandise and convenience foods, through the Company's pharmacy.
The Pharmacy is fully licensed and qualified to conduct business in over 40 US States.
Corporate
The Corporate Segment provides management and administrative services to support the Company, and consists of certain aspects of the Company's executive management, corporate relations, legal, compliance, human resources, and corporate information technology and finance departments. In addition, the Corporate Segment supports the costs and operating expenses related to the continued development and exploitation of the Company's proprietary medical diagnostic and monitoring platform and processes, which remains the Company's primary focus.
Management
Parallax is led by experienced veterans from the healthcare, technology, finance and management fields. The Company's disciplined and organized approach is balanced by its optimism for the future, and the opportunities present in the current healthcare market. The Parallax team is grounded in a belief that success in business is built on a combination of research, planning and execution.
6
The Parallax Business Model
In 60 years, healthcare has transitioned from a direct relationship between doctor and patient, to one that has patients separated from their doctors by the introduction of a huge number of stakeholders, ranging from health insurers, employers, pharmacy benefit managers, imaging, diagnostic testing, lawyers, specialists and a plethora of others. The patient and healthcare provider both want the same thing: information, quality of service, transparency, value for their hard-earned dollars, and more time in their day.
Parallax believes that its products and services can provide solutions that mitigate rising costs, reduce waste in spending through transparency, reduce the amount of unnecessary services, and increase the health and wellness of patients before they are sick.
Parallax has developed, acquired and licensed multiple proprietary and exclusive platforms, that provide services and products, across the healthcare continuum. These platforms are designed to allow for multiple points of reciprocal consideration, through innovative business models, that provide patients with increased quality of services and products, at reduced cost of time and money. They also provide healthcare providers with increased access to their patients, the ability to deliver better and more efficient service and increase their income from the services they supply.
Though Parallax's multiple operations are focused in separate vertical markets, Parallax has designed its business model to allow for cross-pollination and reciprocal transfer of value at multiple points in their respective economic food chains.
The Company's business operations currently generate revenue from its compounding, retail and fertility business, and through multiple economic models ranging from cash payment to insurance reimbursement to rebates from pharmaceutical companies.
Products and Services
The Company's products and services range from compound pharmaceutical drugs and infertility medications to retail drugs.
To date, the primary compound products have been transdermal pain medications, which are made up of several different formulas. The pharmacy also sells non-compounded single ingredient transdermal pain medications.
Business Structure
Parallax operates two divisions, ranging from Parallax Diagnostics, the Company's pre-revenue, point-of-care diagnostics company, to a 61-year-old compound pharmacy, generating millions of dollars in annual revenue and operational in over 40 states in the US., that target markets in:
Pharmaceuticals | RoxSan Pharmacy, Inc. |
Medical Diagnostics | Parallax Diagnostics, Inc. |
Each of Parallax's divisions targets a separate vertical market that is synergistic and complement each other and the Company's value proposition. Designed operational cross-over affords Parallax the ability to use built in economies of scale across multiple operating platforms.
The Cross-Over and Cross-Pollination Model
As an example of the Company's cross-over and cross-pollination model, the nationwide sales infrastructure supporting RoxSan, can be utilized by Parallax's Point-of-care Diagnostic system.
·
RoxSan Pharmacy, the compound and retail pharmacy, sells its drugs to doctors in over 40 US states, approximately 3,500 doctors in its client data base, both active and non-active; and
·
Parallax Diagnostics, the point-of-care testing and diagnostics division, will be able to sell their testing platforms and tests to the RoxSan doctors for use with their patients.
At Parallax, management continually strives to identify solutions to the challenges facing the current healthcare system. Parallax is committed to delivering the highest quality products and services to patients, payers, healthcare insurers and stakeholders that are accessible and reasonable, built upon sound business models and economics that are designed to provide for sustainable growth and increased value to the Company's shareholders.
The Company's business strategy is to expand through organic growth, selective synergistic acquisition, and develop, license and or acquire, quality products and or services that complement the Parallax Mission.
Table of Contents
7
The Company believes that the current healthcare system is built on unsustainable models and significant challenges for all the stakeholders in the healthcare system. The Company strives to identify products, services and technologies that deliver solutions that fill a void in the current market for high quality high efficacy products and services delivered at reasonable and rational prices.
The Company's business model is built on identifying opportunities represented by one market vertical that provides for a separate vertical to utilize one or more of its core operations.
ROXSAN PHARMACY, INC.
COMPOUND and RETAIL PHARMACY SERVICES
Overview
RoxSan Pharmacy, Inc. ("RoxSan"), was incorporated on February 16, 1996, in the state of California, and is located in Beverly Hills, California. Prior to its incorporation in 1996, RoxSan was a privately-owned company providing pharmacy services since the early 1960s.
RoxSan is the oldest continuingly operated pharmacy in Beverly Hills and is a well-known commodity to the residents, and:
·
provides Retail Pharmacy, Compound Pharmacy, Infertility, Wellness, Anti-Aging and Sexual Health products and services.
·
has continually operated at same location for 61 years.
·
is located in prime downtown Beverly Hills, CA location.
·
has a staff of 22 employees, including 4 pharmacist, 3 certified compounding technicians and 2 certified fertility technicians.
Retail Pharmacy Services (RPS)
The RPS provides a full range of pharmacy services including retail, compounding and fertility medications.
The RPS generates net revenues primarily by dispensing prescription drugs, through local channels by direct delivery as well as mail order. The RPS also sells a wide assortment of general merchandise, including over-the-counter drugs, beauty and cosmetic products, seasonal merchandise and convenience foods.
The pharmacy is fully licensed and qualified to conduct business in over 40 US States.
Corporate
The Corporate Segment provides management and administrative services to support the pharmacy. The Corporate Segment consists of certain aspects of the pharmacy's executive management, corporate relations, legal, compliance, human resources, and corporate information technology and finance departments.
Operational Structure and New Business Units
Management developed a system of operations that focused on differentiating unique business markets for RoxSan services and developed additional areas of focus. Currently, RoxSan operates four distinct business units comprised of:
· RoxSan Compound Pharmacy ("Compounding") | · RoxSan Anti-Aging ("RoxSan Anti-Aging") |
· RoxSan Fertility Group ("RoxSan Fertility") | · RoxSan Retail Pharmacy ("RoxSan Retail") |
Shortly after RoxSan's acquisition in August 2015, management determined that there were several areas that required immediate attention.
Pharmacy Compliance
Management created the position of Director of Compliance at RoxSan and put a senior pharmacist as the Director. Management developed a strategic plan covering its Regulatory Compliance goals. The first goal was to create foundational standard operating procedures in the filling, processing, and shipping of prescriptions.
Under this program an audit report ("Audit Report") was discovered that was previously discarded by the prior ownership as having "no relevance" as to the results of the findings in that audit. This audit was part of a due diligence requirement imposed by the Company upon the prior owner before the acquisition, which was to have a third-party organization verify that the pharmacy was operating within compliance of state regulatory demands. The Audit Report dated prior to the acquisition, which was discovered in abandoned files, indicated that several areas of operation of the pharmacy were in violation of the most fundamental compliance rules, and strict warnings as to the consequences of what would happen to the pharmacy's licenses if these areas were not immediately corrected. The Seller did not provide this "material" information while in due diligence prior to the acquisition. All areas recommended in the Audit Report to be corrected, were in fact implemented by the current ownership.
8
State Pharmacy Licenses
The former owner had developed a well-documented contentious relationship with the California Board of Pharmacy as well as a number of other states in which the previous owner was accused of regulatory violations. There were states that had suspended RoxSan's Licenses under the prior ownership to operate in their state. The new management began an aggressive program in each state, to appeal to the State Pharmacy Boards to reinstate the licenses. It became apparent that many individual members on several state Boards of Pharmacy, including the California Board of Pharmacy, the Nevada Board of Pharmacy and the Arizona Board of Pharmacy, had an extremely negative perception of the former owner. With the new management entering into the picture, the negative perception became extremely positive toward RoxSan's new ownership, and its new Compliance Program. Thus far, RoxSan has obtained pharmacy licenses in over 40 US states, and is seeking to obtain licensing in the remaining states.
As a result of the efforts of new management, all of these issues were corrected and the pharmacy is currently operating in an entirely new status of having great relations with each of the previously strained relationships with individual state Boards of Pharmacy.
Pharmacy Benefit Management Business
The former owner had created a negative and challenging relationship with Payers and Pharmacy Benefit Management (PBM's) as well as the cancellation of some pharmacy network contracts with PBM contracts that control the approvals for reimbursements for several health insurers. The new management established a plan of action and SOP's to follow as well as address the criteria for contract re-approvals with the PBM's.
RoxSan Pharmacy has become qualified and fully accredited member of FocusScript's Compounding Pharmacy Network enabling RoxSan to participate in the Pharmacy Benefit Management Program for one of the largest health insurers in the United States. As of this update approximately 5% of the Compound Pharmacy's in the US have been able to achieve this accreditation.
A market development has occurred that has produced a payer reaction to the exorbitantly high pricing trends for compound pain medications. That development has affected the viability of the compound pain medication management industry due to rejections and many of the ingredients becoming "non-covered". RoxSan has developed a program to restructure the pharmacy's approach to creating a more "ethically" based pricing structure with extraordinarily high efficacy formularies, and is working with several of the industry's leading PBM's in pursuit of partnership arrangements.
National Accreditation
In addition, under the new management, RoxSan Pharmacy passed the inspection from the Verified Pharmacy Program (VPP) as part of the National Association of the Board of Pharmacy. This was a significant accomplishment, considering that the prior ownership had failed in passing the VPP inspection in the past. Passing the VPP inspection is an exhaustive process requiring high levels of regulatory systems and compliance. This extraordinary accomplishment was achieved in less than one year under the newly restructured operating compliance program under the new ownership, which included strict adherence to documentation retention and categorization.
Human Resources
In addition to the issues outlined above, it was determined that there were also personnel issues that RoxSan's pharmacists, technicians and general operations employees had with the prior ownership. These issues involved compensation, benefits and management style of leadership, which lacked the opportunity for the employees to be empowered to effectively perform their duties. Management also addressed these issues with clarification of job responsibilities, compensation/benefit adjustments including stock option incentives and an overall more inclusive and open communication style of management.
Market Opportunities
Compounding Industry
What is a Compound Pharmacy?
Pharmacy compounding is the art and science of preparing personalized medications for patients. Compounded medications are made based on a practitioner's prescription in which individual ingredients are mixed together in the exact strength and dosage form required by the patient. This method allows the compounding pharmacist to work with the patient and the prescriber to customize a medication to meet the patient's specific needs.
At one time, nearly all prescriptions were compounded. With the advent of mass drug manufacturing in the 1950s and 1960s, compounding rapidly declined. The pharmacist's role as a preparer of medications quickly changed to that of a dispenser of manufactured dosage forms, and most pharmacists no longer were trained to compound medications. However, the "one-size-fits-all" nature of many mass-produced medications meant that some patients' needs were not being met.
Table of Contents
9
Fortunately, compounding has experienced a resurgence as modern technology and innovative techniques and research have allowed more pharmacists to customize medications to meet specific patient needs.
The primary activities of this industry are: | The major products and services in this industry are: |
|
|
· Preparing alternate dosage forms of medication | · Currently unavailable pharmaceutical manufacturing |
· Preparing alternate strengths of medication | · Pharmaceutical application alteration |
· Preparing flavored medication | · Pharmaceutical dosage alteration |
· Preparing medication for patients with allergies or other sensitivities. | · Pharmaceutical ingredient alteration |
There are no major players in the industry. No single pharmacy holds more than 5% of the market share, offering an opportunity for consolidation, which management has continued to explore as a potential strategy to compliment and secure growth.
Despite the Compounding Pharmacies industry experiencing negative media attention due to contaminated compounded prescriptions, it has still proved to be indispensable. For example, compounded medications can address patients' noncompliance with their medication due to offering tastes, routes of administration and dosages that were not otherwise commercially available. Moreover, the burgeoning elderly population has stimulated demand for prescriptions, including compounded medications that were customized to address a patient's needs. However, from October to September 2012, the Food and Drug Administration (FDA) inspected about 150 compounding pharmacies, with 90.0% of facilities inspected having problems. As a result, some industry operators have exited the industry altogether or have contended with costs related to complying with FDA standards.
Nevertheless, the industry has benefited from pharmaceutical manufacturers having drug shortages, enabling the industry to access raw materials and supply medication orders to patients and hospitals. As group purchasing organizations (GPOs), which secure supplies for healthcare providers, control about 72.0% of purchases made by hospitals, according to the Healthcare Supply Chain Association, drug shortages have occurred. Due to GPOs using their market share as leverage to secure low-cost contracts with pharmaceutical manufacturers, some drug makers did not have the incentive to manufacture and stock essential drugs. As a result, industry revenue is expected to grow at an annualized rate of 2.4% to $5.6 billion during the five years to 2015, including 7.3% growth in 2015. This growth has been driven by the number of active drug shortages increasing from 328 in 2010 to 361 in 2013, according to the latest data available from the United States Government Accountability Office. Profit is anticipated to rise from 25.7% of industry revenue in 2010 to 26.5% in 2015, due to the prescription shortage and lack of substitutes for industry products enabling the industry to garner higher prices.
During the five years to 2020, industry revenue is forecast to grow at an annualized rate of 2.6% to $6.4 billion. As the number of physician visits is expected to rise, more individuals will likely be prescribed medications, which may stimulate demand for compounded pharmaceuticals. Overall, the size of this growth will be contingent on how many patients require medications with alternative dosages and strengths.
Key External Drivers
·
Number of pets (cats and dogs)
·
Number of physician visits
·
Regulation
·
Per capita disposable income
·
Number of adults aged 65 and older
Number of Pets (Cats and Dogs)
In addition to developing drug compounds for humans, compounding pharmacies also create specialized drugs compounded for animals. As the number of pets increases, demand for compounding pharmacies rises, as many pet owners will purchase compounded medications to increase animal compliance with flavoring and alternative routes of administration. The number of pets is expected to increase in 2015.
Number of Physician Visits
Consumers who visit doctors more frequently tend to receive more prescriptions and, in turn, purchase more medications. Therefore, patients may require compounded prescriptions to access drug strengths and forms that are not commercially available. The number of physician visits is expected to increase in 2015.
Regulation
The Food and Drug Administration (FDA) is encouraging large-scale operators to register with the FDA and is increasing federal regulations. As healthcare providers are increasingly purchasing compounded medications from FDA-registered and regulated facilities, many operators will choose to comply with regulations to bolster revenue volumes. Regulation is expected to increase in 2015, which represents a potential threat to the industry.
10
Per Capita Disposable Income
Per capita disposable income determines consumers' ability to purchase this industry's products. While prescription products can be essential for health and therefore less susceptible to changes in consumer discretionary spending, some of the industry's offerings, such as medicine flavorings, are subject to changes in disposable income. An increase in disposable income will boost demand for compounding pharmacies. Per capita disposable income is expected to increase in 2015.
Number of Adults Aged 65 And Older
As the population ages, demand for various pharmaceutical products increases. Adults aged 65 and older are more likely to have chronic illnesses than younger demographics, which stimulates demand for prescriptions. Additionally, elderly individuals may require compounded prescriptions to have personalized dosage forms, flavors or medications that comply with their allergies. The number of adults aged 65 and over is expected to increase in 2015, representing a potential opportunity for the industry.
Current Industry Performance
Recently, significant changes have been made in the Compound Pharmacy industry that have made a detrimental impact on the industry, and have changed the RoxSan product mix permanently from its original growth patterns during 2012 through 2014. The huge growth in the industry during these years, especially in transdermal pain creams, has been reduced in size by as much as 90%. The decline is not driven by a lack of demand, as compounding has become an alternative to traditional medications in a major way. The swift decline has been the result of an oversaturation within the industry, and the reaction to the sudden growth by insurance companies and Pharmacy Benefit Management ("PBM") companies.
At the height of the compound industry growth, topical pain medications had grown astronomically, and in the 3 rd Quarter of 2014, the industry reached a tipping point whereby Express Scripts announced that certain ingredients contained in popular compound medications would no longer be covered by their policies. In 2015, most large payers and their PBM's have stopped reimbursing the compounded topical pain creams.
The Company's pharmacist and senior management agree that the pricing of these compounded drugs was too high and have made attempts to obtain "fix price agreements" with the PBM's and insurers. The Company believes, however, that there is still a great opportunity to develop the topical cream pain business, as it is one of the strongest alternatives to opioid usage, which appears to be the default alternative when a patient is faced with not having the pain creams available to them.
In 2015 there were over 5,500 compounding pharmacies in the US that were estimated to generate over $5.5 billion of revenue and $1.5 billion in profits. Compounding has historically been very profitable, with high gross margins on product sales.
Compound Industry Trends
The Compound Industry information that follows was taken from the IBIS World Industry Report OD5706 Compounding Pharmacies in the US, dated January 2015 by Sarah Turk at https://truenaturepharma.com/wp-content/uploads/2016/01/Compounding-Pharmacies-Industry-Report.pdf. The Company encourages all interested parties to read it closely.
During the past five years, the Compounding Pharmacies industry has exhibited growth, thanks to an increase in the number of dispensed prescriptions. As the burgeoning elderly population has dealt with a number of chronic illnesses that require medication, demand for compounded pharmaceuticals has risen. For example, patients have used compounded prescriptions to access medications in alternative dosages, routes of administration, ingredients (due to patient allergies) and flavorings than drugs that were commercially available. Moreover, the shortage or termination of prescriptions from drug manufacturers' product portfolio has stimulated demand for compounded prescriptions.
In the five years to 2015, industry revenue is anticipated to increase at an annualized rate of 2.4% to $5.6 billion, including 7.3% growth in 2015, due to a rise in the number of prescription shortages. For example, according to data from the United States Government Accountability Office, the number of active drug shortages has increased from 328 in 2010 to 361 in 2013 (latest data available), which has benefited some compounding pharmacies because they were able to supply drugs to hospitals and patients that may have otherwise come from another source. Profit is expected to increase from 25.7% of industry revenue in 2010 to 26.5% in 2015, due to the prescription shortage enabling operators to mark up industry product prices.
Pharmaceutical Awareness: Rising Healthcare Awareness and Spending on Pharmaceuticals Benefits Industry
During the past five years, many Americans have purchased pharmaceuticals to treat their health ailments. According to the Pharmaceutical Research and Manufacturers of America (PhRMA), about 3.6 billion prescriptions are dispensed in the United States each year. The US Pharmacopeia Convention estimates that 30.0 million to 40.0 million of those prescriptions are compounded medications. Over the past five years, numerous trends have increased patient utilization rates of compounded medications. For example, rising healthcare awareness and growth in the number of overall physician visits have bolstered demand for prescriptions and provided a boon to the industry. Moreover, as more patients addressed their allergies to certain drugs and their medication preferences, such as medication that have a different dosage strength, route of administration or flavoring than drugs that were commercially available, demand for compounded medications has increased.
Table of Contents
11
A relative lack of regulation has had mixed effects on the industry. For instance, pharmaceutical manufacturers contend with high costs from generating brand awareness and complying with FDA regulations, which incites manufacturers to limit their product portfolio. While many compounding pharmacies opted for regulation to achieve credibility for their compounding process, such as accreditation with the Pharmacy Compounding Accreditation Board to ensure quality and sterility in their compounding facilities, only 163 pharmacies in the United States were accredited in 2013 (latest data available). As a result, costs for complying with regulation are relatively low when compared with pharmaceutical manufacturers. This has enabled compounding pharmacies to address drug shortages with few financial barriers.
As the number of prescription drug shortages grew, compounding pharmacies were able to help alleviate these shortages by having access to raw materials and downstream markets, such as patients and hospitals. For example, according to the Congressional Research Service's (CRS) Compounded Drugs report, 62.0% of hospitals outsourced compounded drugs due to drug shortages, to ensure drug stability (69.0%) and to extend drug shelf life (62.0%).
However, drug shortages have been particularly prominent among sterile injectable generic drugs, which are difficult to compound safely. Compounding pharmacies have recalled some products, due to not meeting the FDA's standards. This trend has further exacerbated the drug shortage. For example, according to data from the CRS, 48.1% of hospitals reported that a shortage of compounded sterile products would have a significant impact on patient care, whereas 16.6% and 11.5% of hospitals reported that it would result in either an inconvenience or a major disruption to patient care, respectively.
Booming Opportunity: As the Growing Elderly Population Requires More Prescriptions, Demand for the Industry Increased
The burgeoning elderly population has provided a boom for the compounding industry. The number of adults aged 65 and older is expected to grow at an annualized rate of 3.4% during the five years to 2015. More elderly patients have visited their physician, which has stimulated demand for prescriptions. Because the burgeoning elderly population has required more prescriptions to address their numerous chronic illnesses, demand for compounded pharmaceuticals has grown. For example, as the number of stroke patients rose, so did the prevalence of dysphagia, or a patient's inability to swallow. As a result of this trend, demand for compounded medications with alternative routes of administration increased.
Additionally, the industry also provides compounded medications for pets. The number of pet owners is expected to grow at an annualized rate of 2.3% during the five years to 2015. Because of this growth, more pet owners will be required to obtain compounded drugs to increase their pet's compliance with medications. For example, pet owners may demand compounded drugs to cater to their pets' individualized needs, such as allergies and complications with the drug's route of administration.
Industry Outlook
During the next five years, the Compounding Pharmacies industry is expected to benefit from more pharmacies addressing negative media attention from contaminated drugs by registering with the FDA. Moreover, as the elderly population will continue to require a high volume of prescriptions, demand for compounded drugs will increase because some patients will require medications with alterative dosages and strengths that are not commercially available.
Furthermore, as prescription drug shortages continue to occur, which may be partly attributable to the termination of drugs by pharmaceutical manufacturers, patients will need compounded medications to address their health ailments and supply their prescriptions. During the five years to 2020, industry revenue is forecast to grow at an annualized rate of 2.6% to $6.4 billion, which can be attributed to need-based demand for industry products and the lack of a viable substitute. Profit is expected to slightly rise from 26.5% of industry revenue in 2015 to 27.1% in 2020, due to high sales volumes offsetting costs related to complying with regulations.
Rising Incomes and Aging Americans
Consumers' per capita disposable income is linked to demand for compounded pharmaceuticals. For example, many pharmacy benefit managers (PBMs), which are responsible for processing and paying prescription drug claims, have increasingly limited their coverage of compounded drugs. In 2014, Express Scripts, a major PBM, announced that it would no longer cover about 1,000 active ingredients used by compounding pharmacies. As many PBMs attempt to cut costs in response to the rising cost of prescription drugs, they may lower their coverage of compounded drugs. In particular, in 2012, the National Council on Prescription Drug Programs permitted compounding pharmacies to bill for all ingredients used in the compounded drug, rather than for the most expensive ingredient.
Moreover, although compounded drugs make up a small share of total pharmaceuticals, the cost of compounded drugs made with bulk drug substances, such as baclofen (a muscle relaxer) and gabapentin (an anticonvulsant), is rising. In response, PBMs may exclude coverage of industry products. Overall, consumers' per capita disposable income will be a key driver for compounded drugs because many customers will have to pay for industry products out of pocket. In addition, the burgeoning elderly population will provide opportunities for the industry. For example, pharmaceutical manufacturers may produce a drug that does not have the appropriate dosage for elderly individuals, which stimulates demand for compounded medications. Age-related changes, such as medication absorption, distribution, metabolism and excretion, may cause a patient to require compounded prescriptions, bolstering industry revenue.
12
Drug Shortages
Additionally, drug shortages will bolster demand for compounding pharmacies. In 2014 (latest data available), the United States Government Accountability Office (GAO) reported that there was a shortage of about 361 active drugs, which is expected to continue an upward trend over the five-year period. Many drugs included in the shortage were generic sterile injectable drugs. Typically, drug shortages have involved cancer drugs, anesthetics for patients undergoing surgery and electrolytes for patients with intravenous fluids. Consequently, compounding pharmacists that can efficiently manufacture drugs in a sterile environment during a shortage will likely develop favorable supply-side contracts with healthcare providers. Many compounding pharmacies have access to raw materials and can increase their production quickly during a shortage. However, the regulatory landscape will likely become more stringent. More compounding pharmacies have opted to register with the FDA through the Drug Quality and Security Act, giving compounding pharmacies the oversight necessary to develop confidence among healthcare providers and patients. In January 2014 (latest data available), 11 compounding pharmacies have elected to adhere to current good manufacturing standards and FDA inspections, which will likely increase over the five-year period. In particular, sterile compounding facilities, which manufacture drugs that are at high risk for contamination, are expected to increasingly adhere to FDA regulations. With FDA inspections, compounding pharmacies are considered outsourcing facilities, which enables industry operators to provide industry services in bulk to hospitals and physicians when individual prescriptions are not required.
Industry Life Cycle: The industry is growing
Industry value added (IVA), which measures an industry's contribution to the overall economy, is expected to grow at an annualized rate of 3.2% during the 10 years to 2020. Comparatively, GDP is anticipated to increase at an average annual rate of 2.5% during the ten-year period. While contaminated compounded medications have gained negative media attention, drug shortages have still bolstered demand for compounded prescriptions. As consumers continue to require compounded prescriptions to address allergies, provide alternative routes of drug administration as well as dosages or strengths that were not commercially available, the industry will experience stable need-based demand.
While industry operators will increasingly contend with regulation, registering with the FDA will allow compounding pharmacies to be considered outsourcing facilities, which will enable industry operators to supply hospitals with compounded medications in bulk. As the elderly population requires more medications to address their chronic illnesses, demand for compounded prescriptions will also grow, as operators individually tailor prescriptions to meet a patient's dosage or route of administration needs. As consumers become more aware of their health, more individuals will be willing to incur out-of-pocket costs for compounded prescriptions, which benefits the industry.
Demand Determinants
The main drivers affecting demand for compounding pharmacies are consumer incomes and the population's health. Only 1.0% to 2.0% of consumers suffer from allergies or other conditions that require specialized drugs from compounding pharmacies. In general, these consumers can take the unaltered pharmaceutical, but they use compounding pharmacies to manufacture pharmaceuticals that are easier to take, by altering the flavor or application method. This kind of demand is somewhat sensitive to changes in per capita disposable income; as consumer per capita disposable income declines, more consumers will purchase the standardized manufactured pharmaceutical if it is more affordable. Additionally, health insurance companies do not always reimburse consumers who use compounding pharmacies, which constrains demand for compounded prescriptions when consumers cannot incur high out-of-pocket healthcare costs.
However, most customers of compounding pharmacies require their services regardless of the cost. Demand from these customers moves with the general health of the population. The United States population is aging, with more individuals suffering from numerous chronic illnesses, which stimulates demand for compounded medications.
While many individuals require individually tailored compounded medications, age demographics that are typically noncompliant with medications (individuals aged 18 and younger) and elderly individuals with a plethora of chronic illnesses are the main consumers of compounding pharmacies. For example, younger individuals, under the age of 19, are more likely to require medications with alternative applications, due to not being able to take their medication in pill form or due to preferences for particular flavors. Comparatively, elderly individuals comprise a larger market share due to their numerous health ailments, which increases demand for prescriptions.
Individuals aged 18 and younger
Consumers aged 18 and younger also represent a disproportionately large part of industry revenue, accounting for about 15.0% of total revenue in 2015. Aside from the elderly, young children are most likely to have allergies to pharmaceutical compounds, as well as require a special dosage and application method to increase their compliance with medications. During the next five years, demand for compounded medications from this market segment will increase, as more stringent FDA regulations incite more parents to purchase compounded medications for their children.
Individuals aged 19 to 64
The adult population, aged 19 to 64, makes up 55.0% of industry revenue in 2015. During the past five years, this market segment exhibited stable need-based demand, as many individuals required compounded medications with a specific dye due to allergies or gluten-free ingredients for dietary requirements. Furthermore, this demographic demanded compounded drugs due to their low-cost prices, relative to brand-name pharmaceuticals, and accessibility during drug shortages.
Table of Contents
13
Individuals aged 65 and older
According to the US Department of Health and Human Services, consumers aged 65 and over are estimated to account for about 30.0% of pharmaceutical expenditures, indicating that the senior population is one of the primary markets for compounding pharmacies. This age group has a relatively high drug-prescribing pattern, which is due to the number of chronic diseases and disorders and the limited number of non-drug alternatives. The aging baby boomer population has been a key factor of sustained growth in the Compounding Pharmacies industry. As the average age of the US population continues to increase, the volume of drugs prescribed by doctors continues to rise.
Competitive Landscape
Market share concentration: Concentration is very low
The Compounding Pharmacies industry exhibits a low market share concentration, with no firm accounting for 5.0% of total revenue in 2015. Unlike pharmaceutical companies that mass produce medications, compounding pharmacists individually tailor prescriptions to meet specific patient needs, which limits the industry's ability to benefit from cost synergies from economies of scale.
Profit
In 2015, the Compounding Pharmacies industry is expected to generate a robust profit margin (measured as earnings before interest and taxes), accounting for 26.5% of total industry revenue. While profit margins are high for the pharmaceutical sector as a whole, industry operators typically have higher margins, which can be attributed to the industry offering a specialized service with no direct substitutes. However, profit margins vary according to industry operators' product portfolio and clientele.
For example, compounding pharmacies that utilize a variety of ingredients and dosage forms for more patient clinical conditions, or have upgraded facilities for compounding medications, typically have higher profit margins. Furthermore, industry operators that develop contracts with physicians, hospitals and medical clinics will have higher profit margins, compared with compounding pharmacies that work directly with patients on an individual basis. In particular, pharmacies that provide prescriptions during a long-term shortage of critical medications will have high profit margins until the pharmaceutical supply is revived.
Basis of Competition
Firms in the Compounding Pharmacies industry face moderate competition. Competition within the industry stems only from other regionally located firms, due to the industry providing services that lack substitutes. While operators compete on the basis of price, the industry will increasingly generate clientele on the basis of reputation. For example, while the industry is becoming more exposed to regulation, the industry is still experiencing negative media attention from patient deaths and illnesses related to contaminated compounded medications. As a result, industry operators that can generate positive word-of-mouth for compounded medications that are manufactured in sterile environments will likely have a large customer following. Industry operators that develop safe compounded medications that are known for their efficacy will generate high sales volumes. Furthermore, more operators will move toward opting to register with Pharmacy Compounding Accreditation Board and the US Food and Drug Administration's current good manufacturing practices to meet standards for quality in the compounding process.
Compounding pharmacies that are prone to regulation will have an advantage over nonregulated industry operators, which will benefit regulated compounding pharmacies in securing favorable contracts with local physicians, hospitals and medical clinics. Additionally, compounding pharmacies will compete to respond to address shortages of manufactured medications for critical conditions or illnesses, which will benefit operators that have the large compounding facilities and access to raw drug ingredients necessary to manufacture drugs during a shortage. Operators also compete to develop networks with physicians and the healthcare sector, which will benefit operators when patients are referred to compounding pharmacies for specialized medications that are compatible with their allergies, medication strength or other customized prescription needs. Moreover, industry operators also compete to develop networks with downstream industries, such as veterinarians, to be referred when a pet owner requires a compounded prescription for their pet.
Barrier to entry
New entrants to the Compounding Pharmacies industry face moderate barriers to entry. The largest barrier to entry for potential industry entrants includes hiring a specialized work force, which is typically comprised of lab technicians and a pharmacist. Employees must be trained in how to handle and manufacture pharmaceutical products, and firms face competition in hiring employees from traditional pharmaceutical manufacturers and pharmacies. Additionally, compounding pharmacies that specialize in sterile compounding, such as the preparation of injectable drugs and medication that goes into patients' body cavities or sterile areas, incur higher costs for purchasing equipment and maintaining a sterile environment to lower the risk for contamination.
Furthermore, sterile compounding operators also potentially incur costs related to liability issues, which could pose as a potential barrier for potential industry entrants. Many compounding pharmacies have networks with major healthcare systems, which poses as a barrier to entry for small, boutique compounding pharmacies that appeal to local clientele and want to work with healthcare providers. While Accreditation with the Pharmacy Compounding Accreditation Board, which allows operators to achieve legitimacy via regulated operations, can allow potential industry entrants to secure contracts with hospitals, fewer than 5.0% of compounding pharmacies nationwide achieve accreditation, which could limit a compounding pharmacy from entering the industry.
14
In addition, compounding pharmacies must invest in facilities, including a sterile laboratory, suitable for manufacturing pharmaceuticals. Finally, compounding pharmacies typically operate solely in small geographic regions and compete against other industry operators within that region. For a new entrant to be successful, it must find a region in which the existing compounding pharmacies are not meeting the demand from a small customer pool. While being monitored by the FDA is not required for industry operators, many will choose to comply with regulations to build legitimacy and attract healthcare providers. According to MediFare consultants, it costs the average compounding pharmacy facility $35,000 to comply with FDA regulations, which is a significant fixed cost for industry entrants.
Fertility Industry
The market for IVF drugs in California is the largest in the country and is driven my multiple factors as noted above. In addition to the IVF Market information below, sourced from Harris and Williams and Co. a middle market investment advisory and M & A transaction firm, management at RoxSan and its staff, all the way down to the driver delivering the IVF drugs to its customer, are proud to be part of a business that brings children to people who truly want them and have, until their successful treatment for infertility, been unable to conceive on their own. The IVF group at RoxSan is a major factor in the Company's self-esteem, and it is a symbol of pride for everyone that works at RoxSan and Parallax.
Market outlook of the global fertility services market
Market research analysts predict the global fertility services market to grow steadily at a CAGR of nearly 9% between 2016 and 2020. The increase in fertility complications is one of the major drivers for the growth of the market. With age, human body starts undergoing various medical and hormonal changes. Likewise, infertility among women is also an age-related issue. Medically, women above the age of 35 are vulnerable to fertility complications. About 20% of women in the age range of 35-44 undergo fertility services to increase their chances of pregnancy, thus boosting the growth of the fertility services market.
Along with the increase in fertility issues among women, there has also been an increase in the number of fertility clinics worldwide, which is a trending factor contributing to the growth of the market. The rapid rise in the number of fertility clinics is increasing the accessibility of fertility services across the globe, thus facilitating couples to choose clinics based on their convenience.
Segmentation by underlying cause and analysis of the fertility services market
Female infertility is a very common problem in about 10% of women in the age range of 15-44 years. As per the NICE guidelines, female infertility is the inability of a woman of reproductive age to conceive after one year of unprotected vaginal intercourse. Ovulation disorders, submucosal fibroids, pelvic inflammatory disease, and endometriosis are few of the factors that can cause infertility in women.
.
·
15% of the world's population experiences some sort of difficulties conceiving naturally in their life.
·
In the western society, people are prolonging having our first child more and more, which has a clear negative correlation with chances of conceiving naturally.
·
Furthermore, other western lifestyle diseases such as obesity also have a clear negative correlation with natural conception chances.
PARALLAX DIAGNOSTICS, INC.
TARGET SYSTEM and DIAGNOSTIC TESTING PLATFORM
Overview
Parallax Diagnostics, Inc. ("PDI" or "Parallax Diagnostics") is a company focused on the development of point-of-care diagnostics, with an emphasis on its Target System testing platform and novel applications, that detect and/or monitor infectious diseases, cardiac markers and drug of abuse assays. PDI holds exclusive licenses, in perpetuity, to a line of proprietary, patented and/or patent-pending, previously FDA cleared, point-of-care diagnostic tests to be utilized with its single platform diagnostic testing Target System. PDI, with its products and products in development, offers the potential to transform the diagnostic landscape by transitioning critical tests from the centralized lab directly to the hands of the physician or clinicians.
The PDI product line includes an FDA cleared 510K desktop analyzer for both qualitative and quantitative assays and twenty-four FDA 510K-cleared tests for commercial sale in the U.S. PDI also has HIV 1 & 2 tests ready for clinical trial, and a novel CD4-CD8 rapid immune status test targeting the HIV/AIDS/TB treatment and monitoring market.
PDI is currently at a pre-revenue stage, and has spent the last few years prosecuting its patents, as well as initiating development of two (2) CD4-CD8 immune status tests, and the SPARKS Mobile diagnostic reader. PDI also has a technology that was previously cleared by the FDA technology that is being used as a platform for a test that will detect CD4 and CD8 cells which in turn determine a patient's immune status.
The PDI business model is focused on the commercialization of its proprietary diagnostic device in the areas of infectious diseases, cardiac markers, drugs of abuse tests and various other medical conditions.
Patents on its target system diagnostic test platform and test cartridges were issued in the United States, China, Macao, and Hong Kong and its India patent is pending.
Table of Contents
15
The 2015 World market for Point-of-care Testing ("POCT") totaled $22.9 billion.
History of the PDI Target System Technology
The Target System represents the core technology of PDI's point-of-care business.
1982
The Target System was developed and produced by the late Dr. James Parker. In January 1982, James Parker founded V-Tech, Inc. a biomedical and Plastics Company, combining established immunodiagnostic technologies with innovative medical plastic products ("V-Tech"). Mr. Parker's goal was to develop innovative diagnostic tests and testing systems. During his career, Mr. Parker successfully patented over thirty (30) biomedical related products.
1985
Late in 1985, Mr. Parker expanded V-Tech's capabilities by acquiring Organon Diagnostics' 22,500 sq. ft. facility and technical scientific staff. Under Mr. Parker's direction, the acquisition had an immediate impact on V-Tech's pursuit of its major commitment to translate emerging research concepts into useful diagnostic and health care products.
1986
V-Tech introduced its first product on membrane, the Target HCG Test, in the third quarter of 1986. The commercial success of that first product utilizing membrane technology not only spawned a host of additional new tests introduced between 1988 and 1993 but brought V-Tech to the attention of companies such as Miles Laboratories, DuPont, for whom V-Tech successfully developed tests on membrane for agricultural diagnostics, Difco Laboratories, which joint-ventured the application of several analytes.
1986-2001
Between 1986 and 2001, the Target System was manufactured and marketed by V-Tech to medical distributors, hospitals and various government agencies (D.O.D., and G.S.A.). V-Tech owned and operated two manufacturing and distribution facilities, 38,000 and 48,000 square feet in Pomona and the City of Industry, California, respectively. All development and manufacturing, together with FDA compliance laboratory processes, were conducted at these two FDA certified facilities.
2001-2004
The Target System inventor and V-Tech founder, Dr. James Parker, died in October 2001, of an aneurism, just as PDI was beginning to initiate significant sales. Collegues and family members believe that the anuerism was a direct result of a suspicious circumstances surrounding a fall down an escalator in Paris, France, shortly before Dr. Parker was to give a speech at a international conference of diagnostic professionals. V-Tech was in disarray and lay dormant for a number of years under stewards with non-compatible backgrounds. Victor Parker, Esq., son of James Parker approached Ted Withrow, a financier, biomedical executive, entrepreneur and inventor, to help him continue with his father's vision of providing high quality low cost diagnostics in or outside of a hospital. Subsequently, Mr. Withrow approached Dr. Jorn Gorlach, a successful scientist, entrepreneur, biomedical executive and inventor, to join him in founding a new company charged with the commercialization of the Target System and the fulfillment of Dr. Parker's vision. By expanding and applied innovative development to the existing platform, Messer's Withrow and Gorlach were able to lead the new company, Montecito BioSciences, Ltd. ("MBS") into the development of mobile diagnostic and healthcare platform.
MBS applied for and was granted patents covering its mobile technology and Target System test cartridge, and is currently in the pre-prototype stage of development.. SPARKS Mobile, the handheld, mobile technology, will be a next generation version of the VT-1000 reader, and was put into development along with new product segments and market strategies for the reorganization of the Target System technologies and testing platform into MBS. MBS entered into an exclusive license of 24 FDA 510K cleared tests and the FDA 510K cleared immunoassay reader and an Assignment Agreement for the patented and patent-pending applications covering innovations to the Target System and to the business plan.
16
The following list represents historical distributor that sold. The Target Antigen Detection System Diagnostic Platform, including the TARGET VT-1000 Desktop Analyzer and a number of the Company's FDA approved tests in a commercial setting:
Customer | Location |
1. Columbia Diagnostics | Springfield, VA |
2. Cardinal Healthcare | McGaw Park, IL |
3. Community Family Planning | New York, NY |
4. East Tech, Inc. | Indianhead, MD |
5. Laboratory Supply Corp. | Louisville, KY |
6. Medical Technology Corporation | Somerset, NJ |
7. Accumed | Brooklyn, NY |
8. Owens & Minor | Greensburg, PA |
9. General Medical Corp | Richmond, VA |
10. Physicians Sales & Services | Jacksonville, FL |
11. Troy Biological, Inc. | Troy, MI |
12. Alimenterics, Inc. | Morris Plains, NJ |
13. E.I. DuPont Agriculture Department | Newark, DE |
14. Difco Laboratories | Detroit, MI |
15. United States Defense Department | Washington D.C. |
16. Veterans Administration | Washington D.C. |
17. Tryco, Inc. | Mclean, VA |
18. Allied Signal | Jacksonville, FL |
19. VWR International | Bridgeport, NJ |
20. Arab Circle Healthcare | Saudi Arabia |
21. Bioclone Australia | Sydney, Australia* |
22. Care Diagnostics | Vienna, Austria |
23. Izasa, S.A. | Barcelona, Spain |
24. LMC LTD. | Ankara, Turkey |
25. Transasia Bio-Medicals | Bombay India |
2005
●
Withrow developed a business relationship with Victor Parker, the son of James Parker, the inventor of the Target System and the founder and operator of the business that developed and commercialized it.
●
On October 10, 2005 Withrow joined forces with Jorn Gorlach and formed Montecito Bio Sciences, Ltd. ("MBS") as a Nevada corporation
●
The MBS Business plan was to develop the Target System assets, re-launch the Target System into the market and generate revenue through the commercialization of the Intellectual Property.
●
Event Milestones:
●
Re-evaluated HIV 1 and 2 Test that was ready for clinical trial seeking a 510 clearance.
●
Developed a relationship with head of South African Medical Association who directed MBS away from a rapid HIV 1 and 2 test and focused on the need for a low-cost rapid immune status test to be given as part of the HIV-AIDS Antiretroviral treatment.
●
US and International patent applications were filed to protect the business and its stakeholders.
2008- 2010
●
Roth Kline, Inc. was incorporated on December 30, 2008. The sole Shareholder of Roth Kline, Inc. was Montecito Bio Sciences, Ltd.
●
Roth Kline was formed to facilitate the development and commercialization of the Target System.
●
Roth, Kline changed its name to Parallax Diagnostics, Inc.
●
The development of the Target system, Hand held Analyzer & CD4-8 Test became Parallax ' s primary focus.
Product Strategy
In recent years, there has been a continuing shift from the use of laboratory-based analyzers to point-of-care ("POC") tests that can be performed in a matter of minutes. Unlike the centralized clinical laboratory segment of the diagnostic market, which is mature and highly competitive, the POC market is still in its relatively early stages. According to the recent worldwide research reports, however, such as the 2010 Worldwide IVD Market, by the research firm Kalorama Information, the growth rate of the POC market continues to rise. Although certain simple, single analyte diagnostic tests have been developed, such tests have remained incapable of precise and highly sensitive quantitative measurements. As a result, medical tests that require precise quantization of the target analyte have remained the domain of immunoassay analyzers in the centralized laboratory.
Table of Contents
17
Point-of-care diagnostic kits typically consist of test strips that the health care provider applies a patient's sample to and then reads the strip either visually or with an instrument in order to determine a result. They are simple to use, fast, disposable and reliable within an acceptable range. More sensitive analytes or tests requiring quantitative analysis and definitive antibody screening needed in most situations, must be sent out to a diagnostic lab, and hours or days later results arrive. These tests are comparatively complex, expensive, and time consuming; only centralized diagnostic facilities can manage sample handling and the cost of instruments and reagents. A point-of-care instrument that has the advantage of a test strip device in terms of ease of use and rapid results along with ELISA-like capabilities for major diseases would circumscribe diagnosis routinely within the course of a patient visit. This could disrupt the current model. The Company is planning to develop just such a device that it intends to sell to doctors and health care providers.
The commercial success of the current generation of small, simple to use diagnostic devices which provide rapid results in POC applications has been limited by their inability to provide precise, highly sensitive, quantitative measurement.
Despite these limitations, the rapid increase in discovery of individual markers of disease processes, coupled with the advancements in rapid detection technologies, has made these tools available to medical professionals on a wide scale and POC diagnostics are quickly becoming a high growth industry.
The Company believes that there is market potential for advanced POC diagnostic products that provide quick and accurate diagnosis during a patient visit, shortening the decision time to medical intervention and minimizing the need for additional patient follow-up, thereby reducing overall health care delivery costs.
The Company's Target System (the systems includes the VT-1000 Desktop Analyzer, the Target Antigen Detection Cartridge and associated reagents) technology addresses these limitations by applying sophisticated immunochemical and optical methods to detect and quantify analytes present in various human specimens, including blood, urine, and feces. Data indicates that sensitivity will be comparable to expensive and complicated laboratory-based analyzers.
The Company also believes that there is growth opportunity for the exploitation of its Target System platform in developing nations and regions such as Africa, India, South America, Eastern Europe, Russia and Asia as well as developed markets of North America and Western Europe. One of the first initiatives to be developed for this market will combine the Company's SPARKS Mobile (a portable hand-held diagnostic analyzer based on the VT-1000 Desktop Analyzer technology, but smaller and more portable), currently in development, with a test for the monitoring of AIDS/TB patients through the use of a proprietary rapid point-of-care immunoassay CD4-CD8 test called PROMISE CD4, also in development.
The Diagnostics Products
The Company's assets will include a previously FDA-cleared VT-1000 Desktop Analyzer and more than a dozen FDA 510(k) cleared diagnostic tests.
The Company's previously FDA-cleared VT-1000 Desktop Analyzer and immunoassay system incorporates a flow-through rapid antigen test platform configuration that has the ability to produce high-performance quantitative blood test results with the ease of rapid qualitative diagnostic strips. The Company has patent applications related to its current and future products, as well as methods for future test development. The Target VT-1000 Desktop Analyzer is ideally suited for rapid development and commercialization of all new tests that may be introduced.
VT-1000 Desktop Analyzer: Quantitative and Qualitative Immunoassay
The Company's VT-1000 Desktop Analyzer was FDA 510(k) cleared and is capable of rapidly detecting qualitative and quantitative data for the Company's FDA-cleared Target Platform tests. The VT-1000 Desktop Analyzer is used for all Target Platform Tests, allowing for clinical personnel to be trained once and also gives consistent results for either qualitative or quantitative testing.
Target Antigen Detection System ("TADS")
The Target Antigen Detection System consists of a unique disposable cartridge with reagents capable of testing multiple test markers, combined with the VT-1000 Desktop Analyzer. The TADS requires a small amount of sample and provides results in minutes. The simplicity of the fully loaded disposable test cartridge and subsequent ease-of-use of the instrument helps to alleviate the technical burden on medical staff and makes patient diagnosis more efficient.
The Company's Target Antigen Detection System is a departure from the standard devices typical to the rapid testing markets. The device is part of the manufacturer's qualitative and quantitative "Target System Diagnostics Platform," which offers an array of improved modifications and features to the traditional qualitative and semi-quantitative flow-through immunoassay test. With its platform uniformity, vacuum pump, absorption layer for sample overflow, and complete compatibility with single and multi-light source reflectometer technology, the TADS cartridge is a unique collection of tests for qualitative and quantitative detection diseases and of conditions.
The Company plans to develop the SPARKS Mobile, a hand-held analyzer unit, similar in size to a mobile phone/PDA, which will be based on the VT-1000 Desktop Analyzer (see Products in Development).
18
TADS Vacuum Control Flow Device
The TADS cartridge utilizes a vacuum technology to deposit specimen samples uniformly on test membranes. The Vacuum Control Flow Device provides a vacuum pump action, which reduces test time and ensures maximum contact with the membrane antibodies. This collection device allows for numerous tests to be incorporated. The vacuum specimen filtration and excess specimen absorption is built right in.
Target System Patent Status: The Target System and certain of its related components were previously issued patents by the United States Patent and Trademark Office ("USPTO"). The following previously-issued patents have expired:
USPTO Patent # | Description | Date Filed in US | Date Expired |
US4,748,042 | Target Ringing & Spotting Machine (method and Apparatus for Imprinting membrane with pattern of antibody) | May 31, 1988 | May 31, 2008 |
US4,797,260 | Target Cassette (Antibody testing system) | January 10, 1989 | January 1, 2009 |
US5,137,691 | Target Cassette with Removable Air Gap (Antibody testing system with removable air gap) | August 11, 1992 | August 11, 2012 |
The Company's Current Technology
The Company currently holds the rights to certain technology related to the VT-1000 Desktop Analyzer and the Target System.
The Company retained the services of the Intellectual Property Network to provide Intellectual Property protection recommendations for all of the Company's Intellectual Property, open patent applications and products, both domestically and internationally. IPN informs the Company and its shareholders of the accurate and current state of the commercial patent pending coverage, and where possible to identify the existence of novel and patentable inventions present in the current innovation initiative. IPN concluded that the Company has a strong patent portfolio protecting its business, and recommended that the Company aggressively proceed with additional patent applications to protect the Company's inventions and innovations.
There can be no assurance that the Company will be granted patents for any of the patent applications it has filed with the USPTO.
For more information on the Company's patent applications, please see the section entitled "Intellectual Property" contained within this Annual Report.
The Company's previously FDA-Cleared Tests in the area of Infectious Diseases
Rubella
Rubella, German measles, is a highly contagious disease, which is generally transmitted by direct contact with infected persons. Rubella is generally a mild disease. However, when a pregnant woman becomes infected with rubella, the virus may infect the placenta, multiply and induce serious damage to the fetus. Rubella and congenital rubella syndrome became nationally notifiable diseases in 1966. The largest annual total of cases of rubella in the United States was in 1969, when 57,686 cases were reported (58 cases per 100,000 populations). Following vaccine licensure in 1969, rubella incidence fell rapidly. By 1983, fewer than 1,000 cases per year were reported (<0.5 cases per 100,000 population). A moderate resurgence of rubella occurred in 1990-1991, primarily due to outbreaks in California (1990) and among the Amish in Pennsylvania (1991). In 2002 a record low annual total of 18 cases were reported.
Rotavirus
Human rotavirus is recognized as a major cause of gastroenteritis in infants, young children, and the elderly. During the winter months a portion of gastroenteritis in children is due to rotavirus infection. The disease manifests with the symptoms of vomiting, diarrhea, and fever. Rapid and accurate diagnosis is important to avoid inappropriate antibiotic therapy, provide proper treatment early, and to prevent spread of nosocomial infection.
Globally, rotavirus accounts for an estimated 125 million cases of diarrhea each year and represents 30% - 40% of hospitalizations for diarrhea in children less than five years. In developing countries, between 600,000 and 800,000 children die from rotavirus each year (or approximately 2,000 children each day.) This accounts for about one quarter of the deaths from diarrhea and about 5% of all deaths among children less than five years of age.
CMV- Herpes
Cytomegalovirus (CMV) is a human viral pathogen belonging to the Herpes family. Infection in humans is widespread and usually results in asymptomatic disease. However, severe symptomatic infections are a very significant risk in infants and Immuno-compromised individuals. An important primary source of such infection is via blood transfusion and allograft transfer. The serological status of donor and recipient is, therefore, important in patient management.
Table of Contents
19
The United States is not unique in its high rates of CMV seroprevalence. Virtually every country in the world presents similar numbers. Since recurrences are often mild and few patients are aware that they are infected, the infection is likely to continue to rise at double-digit rates without an intervention.
Group A Streptococci: Strep A, Strep Throat, Necrotizing Fasciitis, impetigo
Strep throat is an infection of the pharynx (the part of the throat between the tonsils and the larynx) caused by streptococcus bacteria. The infection is spread by person-to-person contact with nasal secretions or saliva, often among family or household members. Even though the sore throat usually gets better on its own, people who have strep throat should take antibiotics to prevent some of the more serious complications of this infection, particularly acute rheumatic fever.
Approximately 15% of children who have a sore throat and fever are infected by Group A streptococci. CDC estimates that approximately 9,100 cases of invasive GAS disease (rate: 3.2/100,000) and 1,350 deaths occurred nationally during 2002. Disease incidence was highest among children aged <1 year (6.9/100,000) and adults aged >65 years.
Infectious Mononucleosis: EB, Epstein-Barr Viral Syndrome, Mono
Infectious mononucleosis (IM) is a viral infection causing high temperature, sore throat, and swollen lymph glands, especially in the neck. The Epstein-Barr virus typically causes it. Infectious mononucleosis may begin slowly with fatigue, malaise, headache, and sore throat. The sore throat becomes progressively worse, often with enlarged tonsils covered with a whitish-yellow fibrinous exudate. The lymph nodes in the neck are frequently enlarged and painful. Symptoms of mononucleosis gradually subside over a period of weeks to a month. The disease is generally self-limited.
Tests Planned for Development for the Target System Diagnostic Platform
The Company is in the planning process of developing and obtaining FDA clearance for the following products. There can be no assurance that the Company will be successful in developing such tests or in obtaining the required FDA clearance.
HIV 1 & 2 TADS Rapid Test
Today, 42 million people are estimated to be living with HIV/AIDS. Of these, 38.6 million are adults. 19.2 million are women, and 3.2 million are children under 15. During 2002, AIDS caused the deaths of an estimated 3.1 million people, including 1.2 million women and 610,000 children under 15. With the recent advent of Rapid HIV testing, HIV detection and prevention programs around the world have become increasingly effective by reducing their time and costs of detecting the virus, thus allowing for a far greater number of individuals to be screened. The FDA has approved several rapid Immunoassay tests for the detection of HIV, but none of these tests are designed for HIV 1 and 2. The current "rate" of these "rapid" tests is from 15 minutes to hours and only a few can produce results less than 15 minutes.
Additional Products Planned for Development
The Company also believes that there is growth opportunity for the exploitation of the Target System platform in developing nations and regions such as Africa, India, South America, Eastern Europe, Russia and Asia as well as developed markets of North America and Western Europe.
One of the first initiatives for the development of this specific market will be to combine the SPARKS Mobile, the Company's hand-held analyzer (the portable version of its VT-1000 Desktop Analyzer), with a test for the monitoring of HIV/AIDS patients and Tuberculosis patients, through the use of the Company's proprietary rapid POC immunoassay PROMISE CD4 quantitative test, also planned for development.
The Target System Hand-Held Analyzer: SPARKS Mobile
The Company's next generation Target System Analyzer, the SPARKS Mobile, a hand-held analyzer, will include a small, rapid testing format, in conjunction with a hand-held data acquisition and test reading device. The SPARKS Mobile will be a re-engineered version of the Company's previously FDA-approved VT-1000 Desktop Analyzer.
Whether searching for markers in the blood stream, or diagnosing a pathogen in urine, the Company's SPARKS Mobile will be a portable tool for rapid diagnostics. The SPARKS Mobile will also provide an improvement in POC diagnostics and applications in countries with limited health care infrastructures and geographic limitations, both of which are of paramount importance in the combat against infectious diseases and in the fight against proliferation of endemic and pandemic diseases.
This innovative SPARKS Mobile will allow for a fast (minutes instead of hours or days) performance of tests at the point-of-care, and will only require a test cartridge and a small number of ready-to-use solutions in preformatted quantities. Moreover, the SPARKS Mobile will include the ability to store patient information, test data, and QC data, and transmit data through wireless connections.
20
The SPARKS Mobile design goals will plan to:
a)
achieve a portable monitoring system, which is compatible with proven and reliable ELISA-based target system technology.
b)
expand readout capabilities to provide a mobile testing and monitoring platform.
c)
increase the economy of scale and scope of the diagnostics and monitoring platform by the development of additional utility of the device without redundant infrastructure investments (additional data acquisition of patients, additional tests for other, predominant diseases).
The basic design of the Company's SPARKS Mobile is based on the same 510(k) cleared technology employed in its VT-1000 Desktop Analyzer and is compatible with existing Test Cartridges. However, a number of innovative features will be integrated into the design to meet customer and patient needs:
1.
High Infrared Light Spectrum : Multiple light source system providing variable light wave analysis into the infra-red spectrum. This diversity in light source and detection will allow for the simultaneous identification and diagnosis of a broader spectrum of different targets within the same sample and assay. It will also allow for very specific test development, without having to develop a new analyzer to read the results.
2.
Easy Field Upgrades : Field software upgrades made through memory chip (SIMM) or Flash memory stick.
3.
No Change of Equipment : The same Analyzer will be used for all Target System Tests (example: Cardiac Panel., infectious disease), and will be able to be used on all future tests, allowing for training personnel only once, and displaying consistent test results on an easy to read LCD screen.
4.
Printer Hook-up Capability : When hooked to a printer, the SPARKS Mobile will be able to provide printed results for any Target System Test, both Qualitative (when written results must be stored with original test for HIPPA and other compliance issues), or Quantitative (measured amount analysis must be printed and maintained in the patient chart folder).
5.
Low Entry Cost for New Test Development and Analysis : Due to the technologies' broad capability, a new analyzer will not have to be developed for different samples types (blood, serum, plasma, urine, soil or human skin).
6.
Safety, Security and Accuracy by design: For all tests, the SPARKS Mobile bar code activation system will identify the test to be analyzed.
7.
Desk to Docking Station : The SPARKS Mobile will be able to be configured with or without a desk-to-docking station. The docking station will provide a stationary platform when in use in an office or non-mobile application. It will also provide the user to set up multiple tests samples while the analyzer is processing tests.
8.
Smart Phone Capability: The SPARKS Mobile will have many Smart Phone Capabilities including, but not limited to, Bluetooth, WiFi, MMS messaging, SMS, Memory Cards, internal memory expandable to 8GB, data transfer, and more.
PROMISE CD4: CD4-CD8 Rapid Monitoring Test
The Company initiated the development of the CD4-CD8 monitoring rapid test using an immunoassay test the Company has named PROMISE CD4, which the Company believes has the potential to enhance the testing, monitoring and treatment of AIDS patients in developing economies such as South Africa, Sub-Saharan countries, India and other nations struggling to deal with the treatment of AIDS.
AIDS Diagnostics and Immune Status
The Company's aim is to use markers for a disease progression instead of using the cell count method that is associated with and based on those markers. The PROMISE CD4 will include quantification of CD4-CD8 protein in either total blood or CD3 + pre-selected cell populations. This quantification can directly be used to assess an individual's immune status.
AIDS Immune Status: Value Proposition
The treatment of AIDS patients represents a challenge in the developed world and much more so in developing countries. The current methodology to determine the status of an HIV-positive individual involves elaborate technologies to determine the immune status of an individual as well as the presence of the HIV virus in the individual's blood (called the "viral load").
Table of Contents
21
Determination of the immune status is usually performed through so-called cell counts of T-cells, in particular the determination of CD4 + cell count or the relationship of CD4 and CD3 positive cells. This diagnostic procedure requires high-tech machinery (e.g. cell counters), and well-educated laboratory personnel in a stationary laboratory setting. In addition, the cell counting method presently employed and defined by the Western medical community as the "Gold Standard" has shortcomings, which limit its reproducibility and reliability. These factors might cause changes in diagnostic procedures even within those communities in the future. The determination of the amount of virus populating the blood of a person infected with HIV is currently performed through quantitative PCR, again a method requiring stationary settings, as well as highly educated personnel and sophisticated machinery. These setting are usually not available in developing economies. While, in the Western economic environment, the medical care of HIV positive individuals and AIDS patients involves a combination of the above mentioned medical diagnostics in combination with additional, patient dependent procedures, the situation in developing countries looks to the contrary. In South Africa, the country with one of the highest infection rates with HIV in the world, treatment is only available to a small number of infected people. Even under those medication-limited circumstances, treatment is usually administered without any diagnostic procedures concerning the immune status or the viral load of an individual in question, leading to unnecessary treatment of otherwise non-immuno-compromised individuals and the lack of treatment for others with AIDS at later progression. Countries like China have only recently begun to diagnose for HIV positive individuals, and have not moved into the AIDS diagnostic either. The same can be said for many other countries in Africa and Asia.
Requirements for "appropriate" AIDS diagnostics have been defined by many national and international, organizations, amongst them the World Health Organization ("WHO"), under strong influence of scientists mainly from the US and the EU. These requirements have led to the above described situation in developing counties: No appropriate diagnosis of AIDS patients caused by requirements that cannot be achieved under the given circumstances and a strong increase of HIV infection in most of these countries over the last years.
Furthermore, the lack of financial resources are limiting to the expansion of suitable points of diagnostics. Cell counts require elaborate machinery (like FACS or alike) and there are no low-cost or highly portable testing systems available to date. There is an overwhelming demand and urgent need to reduce the costs for cell counting or other methods to determine the immune status, and to increase their usefulness in non-laboratory settings.
In addition, the geographic and social structures of many countries require a more POC oriented approach, as opposed to the dominating centralized care found in highly populated countries in North America and Europe. Therefore, it would by highly desirable to reduce the measurements used as a guide for disease progression or treatment to more simple technologies, like an ELISA performed on a handheld device or similar.
For the Company and its efforts to design a handheld diagnostics device for optimal market use, this means:
·
development of a testing system which is compatible with proven and reliable ELISA based target system technology.
·
expansion of the capabilities of handheld device to provide a mobile testing platform.
·
increase the economy of the diagnostics platform by the development of additional utility of the device without redundant infrastructure investments (additional data acquisition of patients, additional tests for other, predominant diseases).
·
acceptance of the Company's testing system as well as the platform within the medical community of African, Asian, and other countries with mounting problems in the field of HIV and other infectious diseases.
Tests for Other Diseases
The Company's testing system is not limited to HIV or AIDS diagnostics. The test format has been applied in the past to viral and bacterial infections (e.g., Rubella, Rotavirus, Strep. A), and can be adopted toward other epidemics. Diseases like malaria, cholera, hepatitis, yellow fever, or West Nile virus and other viral diseases present increasing health threats to large populations in the world, with major existing problems at the stage of proper diagnosis. The Company believes that it can adapt its VT-1000 Desktop Analyzer and SPARKS Mobile to the rapid, simple, point-of-care diagnosis of almost all of these diseases without the requirement of additional equipment. Further, the Company believes that the combination of a mobile, hand-held testing device with a large number of different tests provided by a family of cartridges will improve the ability of current health care and disease diagnostics in a fast majority of today's underserved regions. In addition, the Target System Platform also allows for the monitoring of environmental components influencing the health of populations, including the presence of toxins in soil and drinking water as well as contamination of food supply.
Ease of Use
The Company's platform provides tremendous flexibility in sample requirements, clinician training and result interpretation. The Company's "train once" system means the clinician can now perform a number of single use tests on a wide variety of conditions with the interpretation of results consistent through the platform paradigm. The "while you watch" speed of the test development, results in a significant cost saving in time and training.
Application and Economy of Scale
The Company's unique vacuum pump action reduces test time and ensures maximum contact with the membrane antibodies. This collection device is versatile in the number of different tests that can be incorporated. The economy of scale is provided to health care provider or any other customer group by being able to utilize a single test system for multiple tests with varies little variance in training needed. A clinician can move from one test to the next in a matter of minutes.
22
Furthermore, the capability of acquiring and transmitting patient related data in addition to the tests performed at the point-of-care will enable the Company's SPARKS Mobile Analyzer to become the central diagnostic device in a decentralized, patient oriented, and cost-conscious environment to provide or maintain a high level of health care in the face of threatening epidemics.
Safety and Accuracy by Design
For all tests, the Company's bar code activation system will identify the test to be analyzed, allowing only those medical personnel that possess that test will be aware that it is available. Without the Company's specific Target System Test Cartridge, read by the bar code reader, the analyzer will not calibrate to that test. This precludes mistakes by the user or erroneous results by the device.
Each Test Cartridge bar code must be read to initialize the analyzer, and load the appropriate algorithm from the software table. This provides a level of security for patient related tests and eliminates errors based on operator's mistakes.
The Company will provide a combination of innovative, fast, and inexpensive diagnostic testing products with a highly mobile data collection and transfer test reader. In this regard, the Company's Target System is suitable for rapid, point-of-care testing in almost every environment, which includes emergency situations, remote locations within the US as well as other parts of the world, immediate response teams, personal testing in a home setting, and many more.
Advantageously, many different tests can be performed using the same reader, e.g., either the Company's VT-1000 Desktop Analyzer or its SPARKS Mobile, currently in development, at any location.
Mobility
The Company's mobile testing, data acquisition, and data transmission system being developed is intended to meet the needs for diagnostics in particular in areas where either no structured health care systems exist or where, due to geographic nature and population density and distribution, a more decentralized approach is necessary. The highly mobile test reader can be used in basically all environments, and will be suited to use power sources independent of an electric network (rechargeable batteries, solar panel, running on motor vehicle voltage and power supply). Furthermore, the tests can be performed within short time periods, and do not require the performing medical personnel, the physician, or the patient to return for test results or potential initiation of treatment.
New Product Screening Criteria
The Target System Platform is broken down into three categories and their associated sub-groups. The categories are:
1. | Qualitative |
2. | Quantitative |
3. | Specialized |
The following list represents a general representation of targeted test to be developed in the area of infectious or highly contagious diseases:
· | Trichomoniasis |
· | Chlamydia |
· | Gonorrhea |
· | Genital herpes (herpes simplex virus of JSV) |
· | Genital warts (human papilloma virus or HPV) |
· | Hepatitis B |
· | H. pylori |
· | Human immunodeficiency virus (HIV) |
· | Lyme Disease |
· | Rocky Mountain Spotted Fever |
· | West Nile |
Raw substances as well as fully developed and commercially available disease markers and antibodies for the diseases listed above as well as many others can be purchased by the Company from a variety of sources and incorporated into the Target System Platform.
This in no way represents the complete segment of Qualitative or Semi-Quantitative tests available for rapid development on the Target System Platform.
Table of Contents
23
New Product Identification
·
Track all CDC, FDA, WHO, relevant reports of medical diagnostic requirements. Provide analysis of whether the test should be Specialized, Quantitative or Qualitative.
·
Determine human capital requirements: project management, outsourcing needed political needs (if any) and social needs (affiliations with association or non-profit groups).
·
Determine the market size and utilization of device needed to address identified diagnostic needs.
·
Determine from source venders what antibodies and antigens are available to use in the Company's device with minimal regulatory and manufacturing hurdles.
·
Perform cost analysis of device manufacture, to include: regulatory application time estimates, clinical requirements, third party and vendor involvement for regulatory support.
·
Identify and prepare pre-market distributor (government or commercial) analysis for market penetration timetable and/or government contract fulfillment.
·
Identify new partnership resources if necessary for specialty devices.
·
On all Quantitative Devices, the Company will determine the Biohazard level at which it is to perform its algorithm development. For highly contagious diseases, the Company will outsource its complete process to a certified lab.
·
In the development of standard quantitative test the Company will determine through the protocol process: how many tests must be performed for an I.R.B. for both the algorithm development (quantitative controls for each test process) and the accuracy of the variable light analysis.
·
All new quantitative tests will be videotaped during algorithm development (light source verification and reflectivity of known sample), and equivalency testing (where the Company compares its device to another like kind device).
·
All software developed for the Company's tests, that are not modifications of existing source code, will be previewed via written outline to the FDA.
Market Opportunities
In recent years, there has been a continuing shift from the use of laboratory-based analyzers to more technologically advanced point-of-care tests that can be performed in a matter of minutes. Unlike the centralized clinical laboratory segment, which is mature and highly competitive, the point-of-care market is still a relatively early stage market. Although certain simple single analyte diagnostic tests have been developed, such tests have remained incapable of precise and highly sensitive quantitative measurements. As a result, medical tests that require precise quantization of the target analyte have remained the domain of immunoassay analyzers.
POC Diagnostic Market
Diagnostic tests performed outside the central laboratory or decentralized testing is generally known as point-of-care (POC). Over the years, the increasing introduction of transportable, portable, and handheld instruments has resulted in the migration of POC testing from the hospital environment to a range of medical environments including the workplace, home, disaster care and most recently, convenience clinics.
Moreover, POC test devices have contributed significantly to the growth of the overall diagnostics market over the past 10 years. As more diagnostic manufacturers pursue CLIA waiver status for their POC devices and CE Mark for POC or self-use. At the same time more decentralized test venues invest in non-waived rapid tests and instruments POC testing appears to be headed for an even bigger role in diagnosis and monitoring patient care.
The Global In-vitro Diagnostics market is expected to grow to $69.1 billion by 2017, up from $49.2 billion in 2012. The growth represents a 7% compounded annual growth rate in five years. Self-testing is the biggest trend fueling the growth. The self-testing market is poised to grow at a CAGR of 9.3% from 2013 to 2018, to reach $27.5 billion by 2018.
The growth is being driven by devices aimed at making acute care more efficient. There is a concerted effort to reduce time spent in expensive intensive care units and in the hospital in general. More tests and technologies have been adapted to serve the needs of physician offices and home testing.
The two factors that are significant to the rapid growth of POC testing are technology advancements and health care economics. The development of new and improved technologies has resulted in the ability to make evidence-based medical decisions that improve patient outcomes and reduce patient acuity, criticality, morbidity and mortality. Quicker diagnosis of infectious agents can also permit the earlier prescription of appropriate medications, thereby potentially shortening the duration of illness.
24
Additionally, the economic climate is driving significant changes in the manner in which patients will be tested and how results are delivered. Recent revisions to government regulations, together with growing patient and insurer pressures on hospitals and physicians have increased incentives to reduce overall patient healthcare costs while providing a higher level of care to a greater number of patients. One cost-cutting measure is to reduce the high cost of diagnostic testing carried out in central laboratory sites.
The Target System provides the platform for the development of a series of quantitative tests for important diagnostic applications that can provide results at a patient's bedside, in a doctor's office, in the emergency room, in a clinic, in an ambulance, on the battlefield, on site agri-business locations, rural and economically disadvantaged areas.
The Target System expects to meet the POC diagnostic market criteria as follows:
·
Rapid turnaround time
·
Direct application of a non-critical volume or placement of sample directly into instrument
·
Disposable device or minimal maintenance required
·
Minimal technical expertise required
·
Positive identification and specimen tracking strategy that eliminates specimen identification errors
·
Simple strategy for calibration and QC
·
Transferability of data to the LIS or HIS
·
Agreement of result with accepted "Gold Standard" tests
·
Affordable cost
Immunoassays: Defined
Immunoassays are chemical tests used to detect or quantify a specific substance, the analyte, in a blood or body fluid sample, using an immunological reaction. Immunoassays are highly sensitive and specific. Their high specificity results from the use of antibodies and purified antigens as reagents. An antibody is a protein (immunoglobulin) produced by B-lymphocytes (immune cells) in response to stimulation by an antigen. Immunoassays measure the formation of antibody-antigen complexes and detect them via an indicator reaction. High sensitivity is achieved by using an indicator system (e.g., enzyme label) that results in amplification of the measured product. Immunoassays may be qualitative (positive or negative) or quantitative (amount measured). An example of a qualitative assay is an immunoassay test for pregnancy. Pregnancy tests detect the presence of human chorionic gonadotropin (hCG) in urine or serum. Highly purified antibodies can detect pregnancy within two days of fertilization. Measuring the signal produced by the indicator reaction performs quantitative immunoassays. This same test for pregnancy can be made into a quantitative assay of hCG by measuring the concentration of product formed.
The purpose of an immunoassay is to measure (or, in a qualitative assay, to detect) an analyte. Immunoassay is the method of choice for measuring analytes normally present at very low concentrations that cannot be determined accurately by other less expensive tests. Common uses include measurement of drugs, hormones, specific proteins, tumor markers, and markers of cardiac injury. Qualitative immunoassays are often used to detect antigens on infectious agents and antibodies that the body produces to fight them. For example, immunoassays are used to detect antigens on Hemophilus, Cryptococcus, and Streptococcus organisms in the cerebrospinal fluid (CSF) of meningitis patients. They are also used to detect antigens associated with organisms that are difficult to culture, such as hepatitis B virus and Chlamydia trichomatis. Immunoassays for antibodies produced in viral hepatitis, HIV, and Lyme disease are commonly used to identify patients with these diseases.
Quantitative Immunoassay Analysis
Immunoassays are powerful techniques for understanding the role of specific components in complex systems. They work on the basis of the recognition of a specific component (target X) by an antibody or equivalent (affibody, RNA aptamer, recombinant antibody, etc.), which results in the production of a detectable signal. In most cases immunoassays are qualitative, providing information in terms of signal intensity. What is really wanted, however, is quantitative assay providing information in absolute chemical terms, namely the concentration of target X.
Quantitative Immunoassays would allow:
·
Detection of the absolute concentration of components
·
Reduce inter-assay variation in data
·
Permit successful statistical analysis of smaller sample sets
·
Permits direct comparison of data generated at independent sites or occasions.
Quantitative Immunoassays are simple to construct. They require the simultaneous analysis of experimental (or test) samples and calibration standards. The signal intensity generated by calibration standards of known concentration permits conversion of the signals generated by the test samples into absolute units of concentration.
Calibration curve
A calibration curve (or standard curve) establishes the relationship between the amount of material present and the signal intensity measured. In the case of immunoassays, this would represent the relationship between the epitope concentration and the signal intensity obtained. This relationship is often non-linear, and in many applications displays a dynamic range (or response range) of approximately two orders of magnitude in the concentration of target X.
Table of Contents
25
To perform a Quantitative Immunoassay, a set of "calibration standards" containing the epitope in various concentrations, are deployed in the immunoassay alongside experimental "test samples". Densitometry is performed on all data from the assay, and curve fitting used to define the relationship between epitope concentration and signal intensity. This mathematical relationship is then used to convert the signals generated by experimental samples into concentration of target X, which in the Company's experience is highly accurate.
Molecular Identity of Calibration Standards
For Western Blot applications, a calibration standard is a molecule which contains the epitope feature of an immunoassay covalently bonded to a protein of known molecular weight. Two configurations of this structure are possible (Figure 1), where the epitope structure is either linked to the amino acid backbone (Fig 1a) in the form of a fusion protein or linked to a side chain of a specific amino acid (Fig 1b).
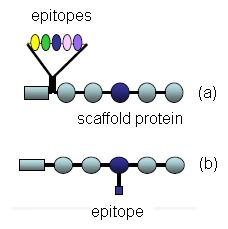
Figure
Figure 1 : Schematic representation of calibration standard molecules.
A set of calibration standards to common epitope tags (His6, c-myc, HA, FLAG, AU1, AU5, glu-glu,) was analyzed by SDS-PAGE/Western blotting (detected via the His6 tag). A single band of 55kDa was detected, and the intensity of signal decreased with decreasing calibration standard loading as expected (Figure 2).
Figure
Figure 2 : Immunodetection of a serial dilution of His6-calibration standard.
Densitometry of the data was performed and the data plotted to define the relationship between epitope amount and signal intensity (Figure 3). Mathematical fitting of the data was performed, with the best fit achieved by "one site-specific binding" analysis (GraphPad Prism) as shown in Figure 3. An excellent fit of the data was achieved using 6 calibration standard concentrations each analyzed in quadruplicate. Similar excellent fits could also be achieved by analysis of fewer standards, with indistinguishable results obtained from 3 calibration standard samples analyzed in triplicate.
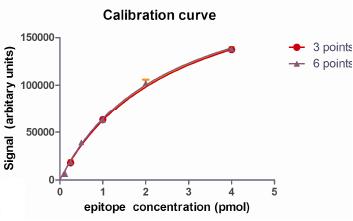
Figure
Figure 3 : Mathematical description of a calibration curve.
To determine the epitope concentration of an experimental sample, the mathematical description of the calibration curve is rearranged to calculate epitope concentration from raw signal intensity. Figure 4 displays the quantitative measurement of three "test" samples. Test samples of 2pmol and 0.5 pmol were analyzed and the results obtained were 2.153± 0.127 pmol (mean ± standard error, n=4), 0.552± 0.045 pmol (mean ± standard error, n=4), confirming the accuracy of the measure (Figure 4). Samples should only be analyzed which fall within the calibration range, as errors are higher for observations beyond the confines of the calibration curve e.g. 0.125 pmol in this example.
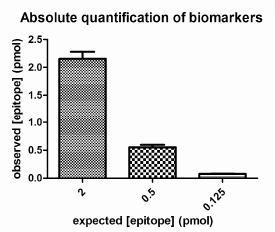
Figure
Figure 4 : Accuracy of Quantitative Immunoassays.
26
In summary, Quantitative Immunoassays are easy to construct and offer several valuable benefits to the researcher. They permit calculation of the absolute concentration of the component of study with high accuracy (error <10%) and high reproducibility. This enhances the quality of research results and also the productivity of research programs by facilitating the direct comparison of data obtained on separate occasions.
The Immunoassay Market
Overview
Immunoassays have been used since the mid-1960's by hospitals, laboratories and research facilities. With the widespread usage of blood and other biological specimen tests for disease and medical condition diagnoses, there is a growing need for new and better technologies to achieve fast and accurate test results. Though the traditional laboratory testing of blood samples has been an acceptable form of screening for certain conditions for quite some time, it has only been in the last twenty years that rapid POC qualitative (yes/no) and semi quantitative (based on predetermined cutoff levels) testing has become an acknowledged source of accurate information.
Rapid Immunoassay Test
With continuing breakthroughs in detectable markers in the body that can identify the presence of a growing number of diseases and conditions, coupled with the advancements in rapid detection technologies, the tools available to medical professionals is quickly becoming a booming industry.
Rapid immunoassays generally come in two configurations: Lateral Flow and Flow-Through. Examples of the rapid immunoassay test are the home pregnancy test and the on-site drug screening test. While both of these examples are based on urine specimens, many of the new rapid screening devices have been developed to use blood as the specimen. The different types of rapid immunoassay test include:
·
Lateral Flow Test
·
Solid Phase Test
·
Agglutination Assay
·
Flow Through Immunoassay
Lateral Flow Tests
A popular testing method used by both professional and over-the-counter tests, the lateral flow test is quick and efficient. Depending on the specific test kit, a sample of urine, whole blood, blood plasma, and in some cases feces, may be mixed with diluting substances, reactive agents or other solutions that are provided for the conduct of the test. Most of the tests are classified as solid phase enzyme immunoassays.
Most home pregnancy tests utilize lateral-flow technology, whereby urine is absorbed through the exposed sample application pad and is allowed (by natural wicking) to migrate to the analytical membrane and react with an embedded agent designed to change color if hormones associated with pregnancy are present in the urine. This is a direct specimen application and does not require dilution or other agents to be added for results to appear. The typical finished product in general use encases all but the application pad in plastic with view openings for the test line or dot and the control line.
Lateral flow devices have been used for home pregnancy tests, drugs of abuse testing in clinical laboratories and, more recently, for home use. Manufactured in continuous membrane strips cut to the desired length and batch tested for accuracy, the manufacture of test kits is highly automated and inexpensive, making lateral flow tests well suited for mass market applications.
Lateral flow devices, however, can suffer in performance when the sample being tested is not handled within strict conditions. Test samples may be affected by environmental conditions (barometric pressure, temperature and humidity), thereby requiring special care in sample preparation, exact dilution controls and controlled time for the test to develop properly. Test development time, for example, can vary from a few minutes (3 to 5) for urine-based tests and up to 20 minutes for whole blood or plasma.
Solid Phase Tests
Solid phase assays include the so-called "dipstick" or "dipstick comb" tests. As its title suggests, the detection materials are in a solid state affixed to a solid, non-porous base. The dipstick is then incubated with the patient's specimen.
The solid phase tests use urine, saliva, serum, plasma, or whole blood as its specimen and the same patient can be tested for multiple parameters with a single assay. Results are usually provided in an hour or less. The sensitivity and accuracy is generally lower than the flow through and lateral flow tests.
Agglutination Test
The basic principle of an agglutination test is the formation of clumps (agglutination) of small particles coated with antigens when exposed to antibodies specific for the antigen. The test particles and the patient antibodies combine to form a visible precipitate. This usually is observed under a microscope.
Table of Contents
27
Some of the advantages of the agglutination test are that its individual test cost is low, the results are semi-quantitative, and it takes a relatively short time to obtain results. However, results can vary as the test reaction depends upon careful control of the test re-agents and environmental conditions. The sensitivity/accuracy is lower than the flow through or lateral flow tests.
Flow-Through Immunoassay
The flow through test procedure requires a number of steps, and includes a vacuum device that deposits fluid containing the test sample through a porous membrane and into an absorbent pad. A second layer, or sub-membrane, inhibits the immediate back-flow of fluids, which can obscure results.
Positive, uniform deposition of test samples on a membrane containing selected diagnostic reagents provides for a flexible, inexpensive and reproducible platform technology to test for a large number of diseases.
The flow-through platform technology can be used to detect both antibodies and antigens. To perform the test, a sample is applied to the membrane followed by a wash step, the addition of the signal reagent, and a second wash to clear the membrane. The solutions can be added as rapidly as the previous liquids are absorbed into the cassette.
The time it takes for a test to display results is subject to the viscosity of the sample, which can be affected by environmental conditions, such as humidity and barometric pressure, further interfering with the time the test takes is the amount of sample used.
Limitations
Each of the screening devices described above have limitations in their utility and range of application. Many screening devices have been adopted from their use in clinical laboratories and, when applied to POC application, required special handling of the specimen samples (blood, urine, and feces) and decreased sensitivity and/or specificity.
Competition
There are approximately 40 to 50 companies in the point-of care ("POC") diagnostic industry in the U.S. and approximately another 100 outside the U.S. The POC space can be broken down into various sub-sets such as molecular biologist developing reagents, and markers to diagnostic equipment and test development companies, as well as companies who do neither and focus on marketing tests, equipment and assays. Most notably in the POC space are the large pharmaceutical companies such as Bayer, Roche, Abbot Labs and others. The Company's specific competitive landscape is tied to its patent pending process involving its SPARKS Mobile Analyzer and Target System Platform In-Vitro Tests. There are a number of companies developing mobile devices to perform a host of health industry-related services and the Company believes that more companies will enter the mobile diagnostic space in the next few years. The industry has yet to develop a standardized point-of-care immunoassay platform for any device to be integrated into. The goal of the Company's SPARKS Mobile Analyzer is to deliver a device that adds immediate value to health providers, patients and health insurance companies. The Company's primary goal is to create a mobile platform that could integrate and utilize the flow-through process of the Company's Target System Platform and offer the healthcare provider a system that is fully interoperable and ubiquitous with a potentially large number of in vitro tests. There are other test platforms in the space but the Company has filed a patent on the process of its SPARKS Mobile Analyzer and its TADS Cartridge. There can be no assurance that the Company's POC device will prove to be competitive with the other POC devices under development.
Until the Company secures a minimum of two million dollars ($2,000,000) of additional capital to operate for the next eighteen months the Company will remain highly vulnerable from the Company's competition. The Company anticipates the need for a minimum of an additional four million ($4,000,000) dollars of investment capital will be required for it to achieve its goal of developing a commercially viable rapid point-of-care CD4-8 immune status test and its proposed mobile SPARKS Mobile version of its FDA Approved VT 1000 Desktop Analyzer. There can be no assurance that such amount will prove adequate to develop the Company' products. Furthermore, the Company's competition has significantly greater resources that it can deploy and anytime to head off competition.
In Vitro Diagnostic Sales Leaders
·
Roche Diagnostics, Switzerland www.roche.com
·
Abbott Diagnostics, Abbott Park, IL 60064 www.abbott.com
·
Siemens Medical Solutions Diagnostics, Deerfield, IL www.diagnostics.siemens.com
·
Johnson & Johnson, Ortho Clinical Diagnostics (OCD) division, Raritan, NJ www.jnj.com
·
Beckman Coulter Inc., Fullerton, CA www.beckmancoulter.com
·
Becton, Dickinson & Co., Franklin Lakes, NJ www.bd.com
·
bioMerieux SA, Marcy l'Etoile, France www.biomerieux.com
·
Bio-Rad Laboraties Inc., Hercules, CA www.bio-rad.com
·
Quidel Inc., San Diego, CA www.quidel.com
·
Alere, Inc. Orlando, FL www.alere.com
28
Barriers to Use
The main barriers and constraints to the use of rapid diagnostic tests can be put into three main categories:
·
Acceptability : Rapid tests need to be acceptable to policymakers, clinicians, and patients. Tests need to have sufficient sensitivity and specificity and need to have an adequate predictive value. Ease-of-use is critical for point-of-care use by clinicians. Culturally appropriate specimens and credible results are important if rapid tests are to be accepted by patients.
·
Affordability: Many rapid diagnostic tests are more expensive than the tests or syndromic algorithms they are intended to replace. Decreasing per-test costs, carefully designing diagnostic algorithms, and educating end users about the cost-savings of more efficient use of therapeutic drugs are important means of maximizing rapid test affordability.
·
Availability: Rapid diagnostic tests are not always available in developing countries. Most tests have limited shelf lives, and many countries have weak public and private sector procurement and distribution systems. The consistency and quality of imported tests can also be issues. To address these constraints, local government regulations, quality assurance, shelf life testing, and distribution systems all need to be assessed and improved. The Company will initially control all of the manufacturing of its Target System test cartridges and Desk Top Analyzer and SPARKS Mobile Analyzer in conjunction with Montecito.
·
Reimbursement : The ability to gain scale in reimbursement across a wide number of test is still a challenge for point of care diagnostic companies such as our Company.
Intellectual Property
The Company's products include a previously FDA-cleared VT-1000 Desktop Analyzer and more than a dozen previously FDA 510(k)-cleared tests. The Company acquired the exclusive rights in perpetuity to a number of pending USPTO Patent Applications on the Company's products in the area of Infectious Diseases, as well as methods for future test development, through a License Agreement with Montecito BioSciences, Ltd.
Parallax intends to seek Intellectual Property protection for all supporting products such as novel biomarker candidates, antibodies, proteins, and diagnostic tests surrounding the Company's core indication areas, in order to create a barrier to entry for its competitors.
The Company retained the services of the Intellectual Property Network to provide Intellectual Property protection recommendations for all of the Company's Intellectual Property, open patent applications and products, both domestically and internationally. IPN informs the Company and its shareholders of the accurate and current state of the commercial patent pending coverage, and where possible to identify the existence of novel and patentable inventions present in the current innovation initiative. IPN concluded that the Company has a strong patent portfolio protecting its business, and recommended that the Company aggressively proceed with additional patent applications to protect the Company's inventions and innovations.
Key Patentable Concepts
·
Sample Analysis
·
Plurality of Isolated Antibodies to a Plurality of Cognate Antigens
·
Identifying Drugs, Targeting Moieties or Diagnostics
·
Determining the Immune Status of a Subject
·
Flow Through Testing System with Pressure Indicator
·
Novel biomarker candidates
·
Antibodies
·
Proteins
·
Diagnostic testing
Parallax / Montecito BioSciences, Ltd. Patents and Applications
Portfolio Overview
Issued Portfolio / Applications Pending or Abandoned
1a. ABANDONED [1] : US11/924,033 "Portable Apparatus for Improved Sample Analysis"