UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE FISCAL YEAR ENDED DECEMBER 31, 2009 |
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission file number: 1-10864
UNITEDHEALTH GROUP INCORPORATED
(Exact name of registrant as specified in its charter)
| MINNESOTA | 41-1321939 | |
(State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) | |
UNITEDHEALTH GROUP CENTER 9900 BREN ROAD EAST MINNETONKA, MINNESOTA | 55343 | |
| (Address of principal executive offices) | (Zip Code) | |
Registrant's telephone number, including area code: (952) 936-1300
Securities registered pursuant to Section 12(b) of the Act:
| COMMON STOCK, $.01 PAR VALUE | NEW YORK STOCK EXCHANGE, INC. | |
| (Title of each class) | (Name of each exchange on which registered) |
Securities registered pursuant to Section 12(g) of the Act: NONE
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes x No ¨
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See the definitions of "large accelerated filer," "accelerated filer" and "smaller reporting company" in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer x | Accelerated filer ¨ | |
Non-accelerated filer ¨ | Smaller reporting company ¨ | |
(Do not check if a smaller reporting company) |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act) Yes ¨ No x
The aggregate market value of voting stock held by non-affiliates of the registrant as of June 30, 2009 was $28,599,603,374 (based on the last reported sale price of $24.98 per share on June 30, 2009, on the New York Stock Exchange).*
As of February 3, 2010, there were 1,157,533,379 shares of the registrant's Common Stock, $.01 par value per share, issued and outstanding.
Note that in Part III of this report on Form 10-K, we incorporate by reference certain information from our Definitive Proxy Statement for the Annual Meeting of Shareholders to be held on May 25, 2010. This document will be filed with the Securities and Exchange Commission (SEC) within the time period permitted by the SEC. The SEC allows us to disclose important information by referring to it in that manner. Please refer to such information.
| * | Only shares of voting stock held beneficially by directors, executive officers and subsidiaries of the Company have been excluded in determining this number. |
TABLE OF CONTENTS
| Page | ||||
| PART I | ||||
Item 1. | Business | 1 | ||
Item 1A. | Risk Factors | 14 | ||
Item 1B. | Unresolved Staff Comments | 25 | ||
Item 2. | Properties | 25 | ||
Item 3. | Legal Proceedings | 25 | ||
Item 4. | Submission of Matters to a Vote of Security Holders | 25 | ||
| PART II | ||||
Item 5. | Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | 26 | ||
Item 6. | Selected Financial Data | 30 | ||
Item 7. | Management's Discussion and Analysis of Financial Condition and Results of Operations | 31 | ||
Item 7A. | Quantitative and Qualitative Disclosures about Market Risk | 50 | ||
Item 8. | Financial Statements and Supplementary Data | 52 | ||
Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure | 94 | ||
Item 9A. | Controls and Procedures | 94 | ||
Item 9B. | Other Information | 97 | ||
| PART III | ||||
Item 10. | Directors, Executive Officers and Corporate Governance | 97 | ||
Item 11. | Executive Compensation | 97 | ||
Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | 97 | ||
Item 13. | Certain Relationships and Related Transactions, and Director Independence | 98 | ||
Item 14. | Principal Accountant Fees and Services | 98 | ||
| PART IV | ||||
Item 15. | Exhibits and Financial Statement Schedules | 99 | ||
| Signatures | 108 | |||
| Exhibit Index | 109 | |||
PART I
| ITEM 1. | BUSINESS |
INTRODUCTION
Overview
UnitedHealth Group Incorporated is a diversified health and well-being company, serving more than 70 million Americans (the terms "we," "our," "us" "UnitedHealth Group" or the "Company" used in this report refer to UnitedHealth Group Incorporated and our subsidiaries). Our focus is on improving the overall health and well-being of the people we serve and their communities and enhancing the performance of the health system. We work with physicians and other health care professionals, hospitals and other key partners to expand access to high quality health care. We help people get the care they need at an affordable cost, support the physician/patient relationship, and empower people with the information, guidance and tools they need to make personal health choices and decisions.
During 2009, we managed approximately $120 billion in aggregate health care spending on behalf of the constituents and consumers we served. Our primary focus is on improving the health care system by simplifying the administrative components of health care delivery, promoting evidence-based medicine as the standard for care, and providing relevant, actionable data that physicians, health care professionals, consumers, employers and other participants in health care can use to make better, more informed decisions.
Through our diversified family of businesses, we leverage core competencies in advanced technology-based transactional capabilities; health care data, knowledge and information; and health care resource organization and care facilitation to improve access to health and well-being services, simplify the health care experience, promote quality and make health care more affordable. These core competencies are focused in two market areas – health benefits and health services. Health benefits are offered in the individual and employer markets and the public and senior markets through our UnitedHealthcare, Ovations and AmeriChoice businesses. Health services are provided to the participants in the health system itself, ranging from employers and health plans to physicians and life sciences companies through our OptumHealth, Ingenix and Prescription Solutions businesses.
Our revenues are derived from premiums on risk-based products; fees from management, administrative, technology and consulting services; sales of a wide variety of products and services related to the broad health and well-being industry; and investment and other income. We have four reporting segments:
| • | Health Benefits (formerly Health Care Services), which includes UnitedHealthcare, Ovations and AmeriChoice; |
| • | OptumHealth; |
| • | Ingenix; and |
| • | Prescription Solutions |
For a discussion of our financial results by reporting segment, see Item 7, "Management's Discussion and Analysis of Financial Condition and Results of Operations."
Additional Information
UnitedHealth Group Incorporated was incorporated in January 1977 in Minnesota. Our executive offices are located at UnitedHealth Group Center, 9900 Bren Road East, Minnetonka, Minnesota 55343; our telephone number is (952) 936-1300.
You can access our website at www.unitedhealthgroup.com to learn more about our Company. From that site, you can download and print copies of our annual reports to shareholders, annual reports on Form 10-K, quarterly
1
reports on Form 10-Q, and current reports on Form 8-K, along with amendments to those reports. You can also download from our website our Articles of Incorporation, bylaws and corporate governance policies, including our Principles of Governance, Board of Directors Committee Charters, and Code of Business Conduct and Ethics. We make periodic reports and amendments available, free of charge, as soon as reasonably practicable after we file or furnish these reports to the SEC. We will also provide a copy of any of our corporate governance policies published on our website free of charge, upon request. To request a copy of any of these documents, please submit your request to: UnitedHealth Group Incorporated, 9900 Bren Road East, Minnetonka, MN 55343, Attn: Corporate Secretary.
Our transfer agent, Wells Fargo Shareowner Services, can help you with a variety of shareholder-related services, including change of address, lost stock certificates, transfer of stock to another person and other administrative services. You can write to our transfer agent at: Wells Fargo Shareowner Services, P.O. Box 64854, St. Paul, Minnesota 55164-0854, email [email protected] , or telephone (800) 468-9716 or (651) 450-4064.
DESCRIPTION OF REPORTING SEGMENTS
Health Benefits
Our Health Benefits reporting segment consists of the following businesses: UnitedHealthcare, Ovations and AmeriChoice. The financial results of UnitedHealthcare, Ovations and AmeriChoice have been aggregated in the Health Benefits reporting segment due to their similar economic characteristics, products and services, types of customers, distribution methods, operational processes and regulatory environment. These businesses also share significant common assets, including our contracted networks of physicians, health care professionals, hospitals and other facilities, information technology infrastructure and other resources. Health Benefits arranges for discounted access to care through a network of approximately 700,000 physicians and other health care professionals and 5,200 hospitals across the United States.
UnitedHealthcare
UnitedHealthcare offers a comprehensive array of consumer-oriented health benefit plans and services for large national employers, public sector employers, mid-sized employers, small businesses and individuals nationwide. UnitedHealthcare facilitated access to health care services on behalf of approximately 25 million Americans as of December 31, 2009. With its risk-based product offerings, UnitedHealthcare assumes the risk of both medical and administrative costs for its customers in return for a monthly premium, which is typically at a fixed rate for a one-year period. UnitedHealthcare also provides administrative and other management services to customers that elect to self-fund the health care costs of their employees and employees' dependants, for which UnitedHealthcare receives a fixed service fee per individual served. These customers retain the risk of financing medical benefits for their employees and employees' dependants, while UnitedHealthcare provides coordination and facilitation of medical services, customer and health care professional services and access to a contracted network of physicians, hospitals and other health care professionals. Large employer groups, such as those serviced by UnitedHealthcare National Accounts, typically use self-funded arrangements. As of December 31, 2009, UnitedHealthcare National Accounts served approximately 380 large employer groups under these arrangements, including 150 of the Fortune 500 companies. Small employer groups are more likely to purchase risk-based products because they are less willing to bear a greater potential liability for health care expenditures. UnitedHealthcare also offers a variety of non-employer based insurance options for purchase by individuals, which are designed to meet the health coverage needs of these consumers and their families.
UnitedHealthcare offers its products through affiliates that are licensed as insurance companies, health maintenance organizations (HMOs), or third party administrators (TPAs). UnitedHealthcare's product strategy centers on several principles: consumer choice, broad access to health professionals, and use of data and science to promote better outcomes, quality service, transparency and affordability. Integrated wellness programs and services help individuals make informed decisions, maintain healthy lifestyles and optimize health outcomes by coordinating access to care services and providing personalized, targeted education and information services.
2
Individuals served by UnitedHealthcare have access to approximately 88% of the physicians and other health care professionals and 96% of the hospitals in the Health Benefits network. The consolidated purchasing capacity represented by the individuals UnitedHealth Group serves makes it possible for UnitedHealthcare to contract for cost-effective access to a large number of conveniently located care professionals. Directly or through UnitedHealth Group's family of companies, UnitedHealthcare offers:
| • | A comprehensive range of benefit plans integrating medical, ancillary and alternative care products so customers can choose benefits that are right for them; |
| • | Affordability across a broad set of price points and a wide product line, from offerings covering essential needs to comprehensive benefit plans, all of which offer access to our broad-based proprietary network of contracted physicians, hospitals and other health care professionals with economic benefits reflective of the aggregate purchasing capacity of our organization; |
| • | Innovative clinical programs that are built around an extensive clinical data set and principles of evidence-based medicine; |
| • | Consumer access to information about physician and hospital performance against quality and cost efficiency criteria based on claims data assessment through the UnitedHealth Premium Designation Program and the UnitedHealth Hospital Comparison Program; |
| • | Physician and facility access to performance feedback information to support continuous quality improvement; |
| • | Care facilitation services that use several identification tools, including proprietary predictive technology to identify individuals with significant gaps in care and unmet needs or risks for potential health problems, and then facilitate appropriate interventions; |
| • | Disease and condition management programs to help individuals address significant, complex disease states; and |
| • | Convenient self-service tools for health transactions and information. |
UnitedHealthcare's regional and national access to broad, affordable and quality networks of health care professionals has advanced over the past several years, with significant increases in access to services throughout the United States. UnitedHealthcare has also organized health care alliances with select regional not-for-profit health plans to facilitate greater customer access and affordability.
UnitedHealthcare's innovation distinguishes its product offerings from its competition. Its consumer-oriented health benefits and services value individual choice and control in accessing health care. UnitedHealthcare has programs that provide health education, admission counseling before hospital stays, care advocacy to help avoid delays in patients' stays in the hospital, support for individuals at risk of needing intensive treatment and coordination of care for people with chronic conditions. To provide consumers with the necessary resources and information to make more informed choices when managing their health, data-driven networks and clinical management are organized through clinical lines of service such as cardiology, oncology, neuroscience, orthopedics, women's health, primary care and emergency services. UnitedHealthcare also offers comprehensive and integrated pharmaceutical management services that promote lower costs by using formulary programs that drive better unit costs for drugs, benefit designs that encourage consumers to use drugs that offer better value and outcomes, and physician and consumer programs that support the appropriate use of drugs based on clinical evidence.
UnitedHealthcare provides innovative programs that enable consumers to take ownership and control of their health care benefits. These products include high-deductible consumer-driven benefit plans coupled with health reimbursement accounts (HRAs), or health savings accounts (HSAs), and are offered on a self-funded and fully-insured basis. UnitedHealthcare provided these products to approximately 24,000 employer-sponsored benefit plans during 2009, including approximately 150 employers in the large group self-funded market serviced by UnitedHealthcare National Accounts.
3
UnitedHealthcare's distribution system consists primarily of brokers and direct and internet sales in the individual market, brokers in the small employer group market, and brokers and other consultant-based or direct sales for large employer and public sector groups. UnitedHealthcare's direct distribution efforts are generally limited to the individual market, portions of the large employer group and public sector markets, and cross-selling of specialty products to existing customers.
Ovations
Ovations provides health and well-being services for individuals age 50 and older, addressing their unique needs for preventive and acute health care services as well as for services dealing with chronic disease and other specialized issues for older individuals. Ovations is fully dedicated to this market segment, as it provides products and services in all 50 states, the District of Columbia, and most U.S. territories. Ovations participates nationally in the Medicare program, offering a wide-ranging spectrum of Medicare products, including Medigap products that supplement traditional fee-for-service coverage, more traditional health-plan-type programs under Medicare Advantage, Medicare Part D prescription drug coverage, and special offerings for beneficiaries who are chronically ill and/or Medicaid and Medicare dual-eligible.
Ovations has extensive capabilities and experience with distribution, including direct marketing to consumers on behalf of its key clients – AARP, the nation's largest membership organization dedicated to the needs of people age 50 and over, state and U.S. government agencies and employer groups. Ovations also has distinct pricing, underwriting, clinical program management and marketing capabilities dedicated to risk-based health products and services in the senior and geriatric markets.
Ovations currently has a number of contracts with Centers for Medicare & Medicaid Services (CMS), which primarily relate to the Medicare health benefit programs authorized under the 2003 Medicare Modernization Act. Premium revenues from CMS were 27% of our total consolidated revenues for the year ended December 31, 2009, most of which were generated by Ovations.
Ovations provides health care coverage for seniors and other eligible Medicare beneficiaries primarily through the Medicare Advantage program administered by CMS. Ovations also offers Medicare Advantage HMO plans, preferred provider organization (PPO) plans, Special Needs Plans, Point-of-Service (POS) plans and Private-Fee-for-Service plans. Under the Medicare Advantage programs, Ovations provides health insurance coverage to eligible Medicare beneficiaries in exchange for a fixed monthly premium per member from CMS that varies based on the geographic areas in which members reside, demographic factors such as age, gender, and institutionalized status, and the health status of the individual. Ovations offers Medicare Advantage products in all 50 states and the District of Columbia. As of December 31, 2009, Ovations had approximately 1.8 million enrolled individuals in its Medicare Advantage products.
Additionally, Ovations provides the Medicare prescription drug benefit (Part D) to beneficiaries throughout the United States and its territories. Among the several Part D plans it offers, Ovations provides Medicare Part D coverage plans with the AARP brand. Ovations provides Part D drug coverage through its Medicare Advantage program, Special Needs Plans (covering individuals who live in an institutional long-term care setting, individuals dual-eligible for Medicaid and Medicare services or individuals with severe or disabling chronic conditions) and stand-alone Part D plans. As of December 31, 2009, Ovations had enrolled approximately 5.9 million members in the Part D program, including approximately 4.3 million members in the stand-alone Part D plans and approximately 1.6 million members in Medicare Advantage plans incorporating Part D coverage.
In association with AARP, Ovations provides a range of standardized Medicare supplement and hospital indemnity insurance offerings from its insurance company affiliates to approximately 3.8 million AARP members. Additional Ovations services include a nurse healthline service, a lower cost standardized Medicare supplement offering that provides consumers with a national hospital network, 24-hour access to health care information, and access to discounted health services from a network of physicians.
4
Ovations also provides complete, individualized care planning and care benefits for aging, disabled and chronically ill individuals. Ovations serves approximately 365,000 individuals (including approximately 255,000 individuals in the Medicare Advantage products) across the nation in long-term care settings including nursing homes, community-based settings and private homes, as well as through hospice and palliative care. Ovations offers services through innovative care management and clinical programs, integrating federal, state and personal funding through a continuum of products from Special Needs Plans and long-term care Medicaid programs to hospice care, and serves people in 35 states and in the District of Columbia in home, community and nursing home settings. These services are provided primarily through nurse practitioners, nurses and care managers.
Ovations also offers a comprehensive eldercare service program providing service coordination, consultation, claim management and information resources nationwide. Proprietary, automated medical record software enables the Ovations clinical care teams to capture and track patient data and clinical encounters, creating a comprehensive set of coherent care information that bridges across home, hospital and nursing home care settings for high-risk populations. Ovations also operates hospice and palliative care programs in 16 local markets in 11 states.
AmeriChoice
AmeriChoice provides network-based health and well-being services to beneficiaries of State Medicaid Children's Health Insurance Programs (SCHIP), and other government-sponsored health care programs. AmeriChoice provides health insurance coverage to eligible Medicaid beneficiaries in exchange for a fixed monthly premium per member from the applicable state. AmeriChoice also offers government agencies a number of diverse management service programs, including a clinical care consulting program, disease and conditions management, pharmacy benefit services and administrative and technology services, to help them effectively administer their distinct health care delivery systems and benefits for individuals in their programs. AmeriChoice also contracts with CMS for the provision of Special Needs Plans serving individuals dual-eligible for Medicaid and Medicare services. These programs are primarily organized toward enrolling individuals who are dual-eligible for Medicaid and Medicare coverage in states where AmeriChoice operates its Medicaid health plans. As of December 31, 2009, AmeriChoice covered 2.8 million beneficiaries through all of its programs in 22 states and District of Columbia.
AmeriChoice's approach is grounded in its belief that health care cannot be provided effectively without considering all of the factors (social, behavioral, economic, environmental, and physical) that affect a person's life. AmeriChoice coordinates resources among family members, physicians, other health care professionals and government and community-based agencies and organizations to provide continuous and effective care. For members, this means that the AmeriChoice Personal Care Model offers them a holistic approach to health care, emphasizing practical programs to improve their living circumstances as well as quality medical care and treatment in accessible, culturally sensitive, community-oriented settings. For example, AmeriChoice's disease management and outreach programs focus on high-prevalence and debilitating illnesses such as hypertension and cardiovascular disease, asthma, sickle cell disease, diabetes, Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS), cancer and high-risk pregnancy. AmeriChoice has developed several of these programs with the help of leading researchers and clinicians at academic medical centers and medical schools.
For physicians, the AmeriChoice Personal Care Model means assistance with coordination of their patients' care. AmeriChoice utilizes sophisticated technology to monitor preventive care interventions and evidence-based treatment protocols to support care management. AmeriChoice operates advanced and unique pharmacy administrative services, including benefit design, generic drug incentive programs, drug utilization review and preferred drug list development to help optimize the use of appropriate quality pharmaceuticals and concurrently manage pharmacy expenditures to levels appropriate to the specific clinical situations.
For state customers, the AmeriChoice Personal Care Model means increased access to care and improved quality for their beneficiaries, in a measurable system that reduces their administrative burden and lowers their costs. AmeriChoice considers a variety of factors when determining in which state programs to participate and on what
5
basis. They include a state's consistency of support for service innovation and funding of its Medicaid program, the population base, the commitment of the physician/provider community to the AmeriChoice Personal Care Model, and the presence of community-based organizations that can partner with AmeriChoice to meet member needs.
OptumHealth
OptumHealth serves nearly 58 million unique individuals with its diversified offering of health, financial and ancillary benefit services and products that assist consumers in navigating the health care system, accessing health services based on their needs, supporting their emotional health and well-being, providing ancillary insurance benefits and helping people finance their health care needs through account-based programs. OptumHealth seeks to simplify the consumer health care experience and facilitate the efficient and effective delivery of care. Its capabilities can be deployed individually or integrated to provide a comprehensive solution oriented around a broad base of consumer needs within the health care system.
OptumHealth's simple, modular service designs can be easily integrated to meet varying employer, payer, public sector and consumer needs at a wide range of price points. OptumHealth offers its products on an administrative fee basis where it manages and administers benefit claims for self-insured customers in exchange for a fixed fee per individual served, and on a risk basis, where OptumHealth assumes responsibility for health care costs in exchange for a fixed monthly premium per individual served. For its financial services offerings, OptumHealth charges fees and earns investment income on managed funds.
OptumHealth distributes its products through three strategic markets: employer (which includes the sub-markets of large, mid and small employers), payer (which includes the sub-markets of health plans, third party administrators, underwriter/stop-loss carriers and individual market intermediaries) and public sector (which includes Medicaid, Medicare and Federal procurement).
OptumHealth is one brand, organized into four major operating groups: OptumHealth Care Solutions, OptumHealth Financial Services, OptumHealth Behavioral Solutions and OptumHealth Specialty Benefits.
Care Solutions. Care Solutions serves more than 40 million individuals through personalized health management solutions that improve people's health and well-being, improve clinical outcomes and workforce productivity and reduce health care costs. Programs include wellness and prevention, disease management, case management, physical health programs, complex condition management, specialized provider networks, personalized health portals and consumer marketing services.
Care Solutions also provides benefit administration and clinical and network management for chiropractic, physical therapy, occupational therapy and other complementary and alternative care services through its national network consisting of approximately 24,000 chiropractors, 16,000 physical and occupational therapists and 8,000 complementary and alternative health professionals.
Financial Services. Financial Services provides health-based financial services for consumers, employers, payers and health care professionals. These financial services include HSAs, HRAs and Flexible Spending Accounts offered through OptumHealth Bank, a Utah-chartered industrial bank. As of December 31, 2009, Financial Services had approximately $860 million in assets under management. Financial Services' health benefit card programs include electronic systems for verification of benefit coverage and eligibility. Financial Services also provides electronic payment and statement services for health care professionals and payers. In 2009, Financial Services electronically transmitted $36 billion in medical payments to physicians and other health care providers.
Behavioral Solutions. Behavioral Solutions serves 43 million individuals with its employee assistance programs, work/life offerings, and clinically driven behavioral health, substance abuse and psychiatric disability management programs. Its consumer-focused programs incorporate state-of-the-art predictive modeling,
6
outcomes management and evidence-based best practices, which result in better care and a reduction in overall health care costs. Behavioral Solutions customers have access to a national network of approximately 87,000 clinicians and counselors and approximately 2,900 facilities in 5,000 locations.
Specialty Benefits. Specialty Benefits includes dental, vision, life, critical illness, short-term disability and stop-loss product offerings delivered through an integrated platform that enhances efficiency and effectiveness. Specialty Benefits covers nearly 23 million individuals and includes a network of approximately 32,000 vision professionals in private and retail settings, and approximately 119,000 dental providers. Stop-loss insurance is marketed throughout the United States through a network of TPAs, brokers and consultants.
Ingenix
Ingenix offers database and data management services, software products, publications, consulting and actuarial services, business process outsourcing services and pharmaceutical data consulting and research services in conjunction with the development of pharmaceutical products on a nationwide and international basis. As of December 31, 2009, Ingenix's customers include approximately 6,000 hospitals, 245,000 physicians, 2,000 payers and intermediaries, 200 Fortune 500 companies, 655 life sciences companies, 350 government entities, and 135 United Kingdom Government Payers, as well as other UnitedHealth Group businesses.
Ingenix is engaged in the simplification of health care administration with information and technology. Ingenix helps customers accurately and efficiently manage the information flowing through the health care system. Ingenix uses data to help advance transparency on cost and quality and help customers streamline their processes to make health care more efficient. Ingenix is a leader in contract research services, and pharmacoeconomics, epidemiology and safety and outcomes (including comparative effectiveness) research through its i3 businesses.
Ingenix's products and services are sold primarily through a direct sales force focused on specific customers and market segments across the pharmaceutical, biotechnology, employer, government, hospital, physician, payer and property and casualty insurance market segments. Ingenix's products are also supported and distributed through an array of alliance and business partnerships with other technology vendors, who integrate and interface its products with their applications.
Many of Ingenix's contract research services, consulting arrangements and software and related information services are performed over an extended period, often several years. Ingenix maintains an order backlog to track unearned revenues under these long-term arrangements. The backlog consists of estimated revenue from signed contracts or other legally binding agreements that either have not started but are anticipated to begin in the near future, or are in process and have not been completed. Ingenix's aggregate backlog at December 31, 2009 was $2.2 billion, of which $1.6 billion is expected to be realized within the next 12 months. This includes $0.7 billion related to intersegment agreements all of which are included in the current portion. Ingenix cannot provide any assurance that it will be able to realize all of the revenues included in backlog due to uncertainty regarding the timing and scope of services and the potential for cancellation or early termination of certain service arrangements.
The Ingenix companies are divided into two groups: Information Services and i3.
Information Services. Information Services' diverse product offerings help clients strengthen health care administration and advance health care outcomes. These products include health care utilization reporting and analytics, physician clinical performance benchmarking, clinical data warehousing, analysis and management responses for medical cost trend management, physician practice revenue cycle management, including integrated electronic medical record systems, revenue and payment cycle management for payer and health care professional organizations, payment accuracy solutions, decision-support portals for evaluation of health benefits and treatment options, risk management solutions, connectivity solutions and claims management tools to reduce administrative errors and support fraud recovery services. Information Services uses proprietary software
7
applications that manage clinical and administrative data across diverse information technology environments. Information Services also uses proprietary predictive algorithmic applications to help clients detect and act on repetitive health care patterns in large data sets. Information Services offers comprehensive Electronic Data Interchange (EDI) services helping health care professionals and payers decrease costs of claims transmission, payment and reimbursement through both networked and direct connection services. Information Services publishes print and electronic media products that provide customers with information regarding medical claims coding, reimbursement, billing and compliance issues.
Information Services provides other services, such as verification of physician credentials, health care professional directories, Healthcare Effectiveness Data and Information Set (HEDIS) reporting, and fraud and abuse detection and prevention services. Information Services also offers consulting services, including actuarial and financial advisory work through its Ingenix Consulting division and health care policy research, implementation, strategy and management consulting through its subsidiary, The Lewin Group, as well as product development, health care professional contracting and medical policy management.
i3. i3 uses comprehensive, science-based evaluation and analysis and benchmarking services to support pharmaceutical and biotechnology development. i3 provides services on a nationwide and international basis, helping customers effectively and efficiently get drug data to appropriate regulatory bodies and to improve health outcomes through integrated information, analysis and technology. i3's capabilities and efforts focus on the entire range of product assessment, through commercialization of life-cycle management services – pipeline assessment, market access and product positioning, clinical trials, economic, epidemiology and safety and outcomes (including comparative effectiveness) research. i3's global contract research services include regulatory assistance, project management, data management, biostatistical analysis, quality assurance, medical writing and staffing resource services. i3's contract research services are therapeutically focused on oncology, the central nervous system, respiratory, infectious and pulmonary diseases and endocrinology.
Prescription Solutions
Prescription Solutions offers a comprehensive suite of integrated pharmacy benefit management (PBM) services to approximately 11 million people, delivering drug benefits through approximately 66,000 retail network pharmacies and two mail service facilities as of December 31, 2009. Prescription Solutions processed approximately 320 million adjusted scripts in 2009 by servicing internal customers in our Health Benefits segment, as well as external employer groups, union trusts, managed care organizations, Medicare-contracted plans, Medicaid plans and TPAs, including mail service only and carve-out accounts.
Prescription Solutions' integrated PBM services include retail network pharmacy management, mail order pharmacy services, specialty pharmacy services, benefit design consultation, drug utilization review, formulary management programs, disease therapy management and adherence programs. Prescription Solutions' products and services are designed to enhance clinical outcomes with reduced costs for those served. The fulfillment capabilities of Prescription Solutions are an important strategic component in serving commercial health plans and Medicare-contracted businesses, including Part D prescription drug plans.
Prescription Solutions' distribution system consists primarily of health insurance brokers and other health care consultant-based or direct sales. In addition to PBM services, Prescription Solutions' Consumer Health Products division delivers diabetic testing and other specialized medical supplies, over the counter items, vitamins and supplements directly to members' homes.
GOVERNMENT REGULATION
Most of our health and well-being services are regulated by federal and state regulatory agencies that generally have discretion to issue regulations and interpret and enforce laws and rules. This regulation can vary significantly from jurisdiction to jurisdiction. Federal and state governments continue to enact and consider
8
various legislative and regulatory proposals that could materially impact certain aspects of the health care system, including proposals to address the affordability and availability of health insurance and to reduce the number of uninsured individuals. The interpretation of existing laws and rules also may change periodically. New laws, regulations and rules, or changes in the interpretation of existing laws, regulations and rules, could negatively affect our business. We believe we are in compliance in all material respects with applicable laws, regulations and rules. In the event we fail to comply with federal and state regulations, or fail to respond quickly and appropriately to health care reforms and frequent changes in federal and state regulations, our business, financial condition and results of operations could be materially adversely affected. See Item 1A, "Risk Factors" for a discussion of the risks related to compliance with federal and state government regulations.
Federal Laws and Regulation
We are subject to various levels of federal regulation. CMS regulates Ovations and AmeriChoice Medicare and Medicaid businesses. CMS has the right to audit performance to determine compliance with CMS contracts and regulations and the quality of care given to Medicare beneficiaries. Our Health Benefits reporting segment, through AmeriChoice and Ovations, also has Medicaid and SCHIP contracts that are subject to federal regulations regarding services to be provided to Medicaid enrollees, payment for those services, and other aspects of these programs. There are many regulations surrounding Medicare and Medicaid compliance. When we contract with the federal government, we are subject to federal laws and regulations relating to the award, administration and performance of U.S. Government contracts. In addition, the portion of Ingenix's business that includes clinical research is subject to regulation by the U.S. Food and Drug Administration. Laws and regulations relating to consumer protection, anti-fraud and abuse, anti-kickbacks, anti-money laundering, securities and antitrust also affect us.
HIPAA, GLBA and Other Privacy and Security Regulation. The administrative simplification provisions of the Health Insurance Portability and Accountability Act of 1996, as amended (HIPAA), apply to both the group and individual health insurance markets, including self-funded employee benefit plans. HIPAA requires guaranteed health care coverage for small employers and certain eligible individuals. It also requires guaranteed renewability for employers and individuals and limits exclusions based on preexisting conditions. Federal regulations promulgated pursuant to HIPAA include minimum standards for electronic transactions and code sets, and for the privacy and security of protected health information. The HIPAA privacy regulations do not preempt more stringent state laws and regulations that may also apply to us.
Federal privacy and security requirements change frequently because of legislation, regulations and judicial or administrative interpretation. For example, the U.S. Congress enacted the American Recovery and Reinvestment Act of 2009 (ARRA) which significantly amends, and adds new, privacy and security provisions to HIPAA and imposes additional requirements on uses and disclosures of health information. AARA includes new contracting requirements for HIPAA business associate agreements; extends parts of HIPAA privacy and security provisions to business associates; adds new federal data breach notification requirements for covered entities and business associates and new reporting requirements to the Department of Health and Human Services (HHS) and the Federal Trade Commission (FTC) and, in some cases, to the local media; strengthens enforcement and imposes higher financial penalties for HIPAA violations and, in certain cases, imposes criminal penalties for individuals, including employees. In the conduct of our business, we may act, depending on the circumstances, as either a covered entity or a business associate. Federal consumer protection laws may also apply in some instances to privacy and security practices related to personal identifiable information. The use and disclosure of individually identifiable health data by our businesses is also regulated in some instances by other federal laws, including the Gramm-Leach-Bliley Act (GLBA) or state statutes implementing GLBA, which generally require insurers to provide customers with notice regarding how their non-public personal health and financial information is used and the opportunity to "opt out" of certain disclosures before the insurer shares such information with a third party, and which generally require safeguards for the protection of personal information. See Item 1A, "Risk Factors" for a discussion of the risks related to compliance with HIPAA, GLBA and other privacy-related regulations.
9
ERISA. The Employee Retirement Income Security Act of 1974, as amended (ERISA), regulates how goods and services are provided to or through certain types of employer-sponsored health benefit plans. ERISA is a set of laws and regulations subject to periodic interpretation by the U.S. Department of Labor (DOL) as well as the federal courts. ERISA places controls on how our business units may do business with employers who sponsor employee benefit health plans, particularly those that maintain self-funded plans. Regulations established by the DOL provide additional rules for claims payment and member appeals under health care plans governed by ERISA. Additionally, some states require licensure or registration of companies providing third-party claims administration services for health care plans.
FDIC. The Federal Deposit Insurance Corporation (FDIC) has federal regulatory and supervisory authority over OptumHealth Bank and performs annual examinations to ensure that the bank is operating in accordance with federal safety and soundness requirements. In addition to such annual examinations, the FDIC performs periodic examinations of the bank's compliance with applicable federal banking statutes, regulations and agency guidelines. In the event of unfavorable examination results, the bank could be subject to increased operational expenses, governmental oversight and monetary penalties.
State Laws and Regulation
Health Care Regulation. Our insurance and HMO subsidiaries must be licensed by the jurisdictions in which they conduct business. All of the states in which our subsidiaries offer insurance and HMO products regulate those products and operations. These states require periodic financial reports and establish minimum capital or restricted cash reserve requirements. With the amendment of the Annual Financial Reporting Model Regulation by the National Association of Insurance Commissioners to adopt elements substantially similar to the Sarbanes-Oxley Act of 2002, we expect that these states will continue to expand the scope of regulations relating to corporate governance and internal control activities of HMOs and insurance companies.
Health plans and insurance companies are also regulated under state insurance holding company regulations. Such regulations generally require registration with applicable state departments of insurance and the filing of reports that describe capital structure, ownership, financial condition, certain intercompany transactions and general business operations. Some state insurance holding company laws and regulations require prior regulatory approval of acquisitions and material intercompany transfers of assets, as well as transactions between the regulated companies and their parent holding companies or affiliates. These laws may restrict the ability of our regulated subsidiaries to pay dividends.
In addition, some of our business and related activities may be subject to other health care-related regulations and requirements, including PPO, managed care organization (MCO), utilization review (UR) or third-party administrator-related regulations and licensure requirements. These regulations differ from state to state, but may contain network, contracting, product and rate, and financial and reporting requirements. There are laws and regulations that set specific standards for delivery of services, payment of claims, adequacy of health care professional networks, fraud prevention, protection of consumer health information, pricing and underwriting practices, and covered benefits and services. State health care anti-fraud and abuse prohibitions encompass a wide range of activities, including kickbacks for referral of members, billing unnecessary medical services, and improper marketing. Our AmeriChoice and Ovations Medicaid businesses are subject to regulation by state Medicaid agencies that oversee the provision of benefits by AmeriChoice to its Medicaid and SCHIP beneficiaries and by Ovations to its Medicaid beneficiaries. We also contract with state governmental entities and are subject to state laws and regulations relating to the award, administration and performance of state government contracts.
Pharmacy Regulation. Prescription Solutions' mail order pharmacies must be licensed to do business as a pharmacy in the state in which they are located. Our mail order pharmacies must also register with the U.S. Drug Enforcement Administration and individual state controlled substance authorities to dispense controlled substances. In many of the states where our mail order pharmacies deliver pharmaceuticals there are laws and
10
regulations that require out-of-state mail order pharmacies to register with that state's board of pharmacy or similar regulatory body. These states generally permit the pharmacy to follow the laws of the state in which the mail order pharmacy is located, although some states require that we also comply with certain laws in that state. Our mail order pharmacies maintain certain Medicare and state Medicaid provider numbers as pharmacies providing services under these programs. Participation in these programs requires the pharmacies to comply with the applicable Medicare and Medicaid provider rules and regulations. Other laws and regulations affecting our mail order pharmacies include federal and state statutes and regulations govern the labeling, packaging, advertising and adulteration of prescription drugs and dispensing of controlled substances. See Item 1A, "Risk Factors" for a discussion of the risks related to our PBM businesses.
Privacy and Security Laws. States have adopted regulations to implement provisions of the GLBA. Like HIPAA, GLBA allows states to adopt more stringent requirements governing privacy protection. A number of states have also adopted other laws and regulations that may affect our privacy and security practices, for example, state laws that govern the use, disclosure and protection of social security numbers. State and local authorities increasingly focus on the importance of protecting individuals from identity theft, with a significant number of states enacting laws requiring businesses to notify individuals of security breaches involving personal information. State consumer protection laws may also apply to privacy and security practices related to personally identifiable information, including information related to consumers and care providers. Additionally, different approaches to state privacy and insurance regulation and varying enforcement philosophies in the different states may adversely affect our ability to standardize our products and services across state lines. See Item 1A, "Risk Factors" for a discussion of the risks related to compliance with state privacy-related regulations.
UDFI. In addition, the Utah State Department of Financial Institutions (UDFI) has state regulatory and supervisory authority over OptumHealth Bank and in conjunction with federal regulators performs annual examinations to ensure that the bank is operating in accordance with state safety and soundness requirements. In addition to such annual examinations, the UDFI in conjunction with federal regulators performs periodic examinations of the bank's compliance with applicable state banking statutes, regulations and agency guidelines. In the event of unfavorable examination results, the bank could be subjected to increased operational expenses, governmental oversight and monetary penalties.
Commitments. In connection with the PacifiCare Health Systems, Inc. (PacifiCare) and Sierra Health Services, Inc. (Sierra) acquisitions, which closed in December 2005 and February 2008, respectively, certain of our subsidiaries entered into various commitments with state regulatory departments, principally in California and Nevada. Many of the PacifiCare commitments in California expired on December 19, 2009. We believe that none of the remaining commitments in any of the affected states will materially affect our operations.
Audits and Investigations
We have been and are currently involved in various governmental investigations, audits and reviews. These include routine, regular and special investigations, audits and reviews by CMS, state insurance and health and welfare departments, state attorneys general, the Office of the Inspector General, the Office of Personnel Management, the Office of Civil Rights, U.S. Congressional committees, the U.S. Department of Justice, U.S. Attorneys, the SEC, the Internal Revenue Service, the U.S. Department of Labor and other governmental authorities. Such government actions can result in assessment of damages, civil or criminal fines or penalties, or other sanctions, including loss of licensure or exclusion from participation in government programs. See Note 14 of Notes to the Consolidated Financial Statements for details. In addition, disclosure of any adverse investigation, audit results or sanctions could negatively affect our reputation in various markets and make it more difficult for us to sell our products and services and retain our current business.
International Regulation
Some of our business units, including Ingenix's i3 business, have international operations. These international operations are subject to different legal and regulatory requirements in different jurisdictions, including various tax, tariff and trade regulations, as well as employment, intellectual property, privacy, and investment rules and laws.
11
COMPETITION
As a diversified health and well-being services company, we operate in highly competitive markets. Our competitors include managed health care companies, insurance companies, HMOs, TPAs and business services outsourcing companies, health care professionals that have formed networks to directly contract with employers or with CMS, specialty benefit providers, government entities, disease management companies, and various health information and consulting companies. For our Health Benefits businesses, competitors include Aetna Inc., Cigna Corporation, Coventry Health Care, Inc., Health Net, Inc., Humana Inc., Kaiser Permanente, WellPoint, Inc., numerous for-profit and not-for-profit organizations operating under licenses from the Blue Cross Blue Shield Association and other enterprises that serve more limited geographic areas. For our Prescription Solutions businesses, competitors include Medco Health Solutions, Inc., CVS Caremark Corporation and Express Scripts, Inc. Our OptumHealth and Ingenix reporting segments also compete with a broad and diverse set of other businesses. New entrants into the markets in which we compete, as well as consolidation within these markets, also contribute to a competitive environment. We believe the principal competitive factors that can impact our businesses relate to the sales, marketing and pricing of our products and services; product innovation; consumer satisfaction; the level and quality of products and services; care delivery; network capabilities; market share; product distribution systems; efficiency of administration operations; financial strength and marketplace reputation. If we fail to compete effectively to maintain or increase our market share, including maintaining or increasing enrollments in businesses providing health benefits, our results of operations could be materially adversely affected. See Item 1A, "Risk Factors," for additional discussion of our risks related to competition.
EMPLOYEES
As of December 31, 2009, we employed approximately 80,000 individuals. We believe our employee relations are generally positive.
EXECUTIVE OFFICERS OF THE REGISTRANT
The following sets forth certain information regarding our executive officers as of February 3, 2010, including the business experience of each executive officer during the past five years:
Name | Age | Position | ||
Stephen J. Hemsley | 57 | President and Chief Executive Officer | ||
George L. Mikan III | 38 | Executive Vice President and Chief Financial Officer | ||
Gail K. Boudreaux | 49 | Executive Vice President of UnitedHealth Group and President of UnitedHealthcare | ||
William A. Munsell | 57 | Executive Vice President of UnitedHealth Group and President of Enterprise Services Group | ||
Eric S. Rangen | 53 | Senior Vice President and Chief Accounting Officer | ||
Larry C. Renfro | 56 | Executive Vice President of UnitedHealth Group and Chief Executive Officer of Public and Senior Markets Group | ||
Lori K. Sweere | 51 | Executive Vice President of Human Capital | ||
Christopher J. Walsh | 44 | Executive Vice President, General Counsel and Assistant Secretary | ||
Anthony Welters | 54 | Executive Vice President of UnitedHealth Group and President of Public and Senior Markets Group | ||
David S. Wichmann | 47 | Executive Vice President of UnitedHealth Group and President of UnitedHealth Group Operations | ||
Mitchell E. Zamoff | 42 | Executive Vice President, General Counsel and Assistant Secretary |
12
Our Board of Directors elects executive officers annually. Our executive officers serve until their successors are duly elected and qualified.
Mr. Hemsley is President and Chief Executive Officer of UnitedHealth Group, has served in that capacity since November 2006, and has been a member of the Board of Directors since February 2000. Mr. Hemsley served as President and Chief Operating Officer from 2004 to November 2006. He joined UnitedHealth Group in 1997 and held various executive positions with the Company from 1997 to 2004.
Mr. Mikan is Executive Vice President and Chief Financial Officer of UnitedHealth Group and has served in that capacity since November 2006. Mr. Mikan served as Senior Vice President of Finance of UnitedHealth Group from February 2006 to November 2006. From June 2004 to February 2006, Mr. Mikan served as Chief Financial Officer of UnitedHealthcare and as President of UnitedHealth Networks. Mr. Mikan was Chief Financial Officer of Specialized Care Services (now OptumHealth) in 2004. Mr. Mikan joined UnitedHealth Group in 1998 and held various executive positions with the Company from 1998 to 2004.
Ms. Boudreaux is Executive Vice President of UnitedHealth Group and President of UnitedHealthcare and has served in that capacity since May 2008. Prior to joining UnitedHealth Group, Ms. Boudreaux served as Executive Vice President of Health Care Services Corporation (HCSC) from December 2005 to May 2008 and as President of Blue Cross and Blue Shield of Illinois, a division of HCSC, from 2002 to December 2005.
Mr. Munsell is Executive Vice President of UnitedHealth Group and President of the Health Services Group and has served in that capacity since September 2007. From December 2006 to August 2007, Mr. Munsell served as Executive Vice President of UnitedHealth Group. From November 2004 to December 2006, Mr. Munsell served as Chief Executive Officer of Specialized Care Services (now OptumHealth). In 2004, Mr. Munsell served as the Chief Administrative Officer and Chief Operating Officer of UnitedHealthcare. Mr. Munsell joined UnitedHealth Group in 1997 and held various executive positions with the Company from 1997 to 2004.
Mr. Rangen is Senior Vice President and Chief Accounting Officer of UnitedHealth Group and has served in that capacity since December 2006. From November 2006 to December 2006, Mr. Rangen was Senior Vice President of UnitedHealth Group. Mr. Rangen joined UnitedHealth Group in November 2006. Prior to joining UnitedHealth Group, Mr. Rangen served as Executive Vice President and Chief Financial Officer of Alliant Techsystems Inc. from April 2004 to March 2006 and as Vice President and Chief Financial Officer of Alliant Techsystems, Inc. from 2001 to April 2004.
Mr. Renfro is Executive Vice President of UnitedHealth Group and Chief Executive Officer of the Public and Senior Markets Group and has served in that capacity since October 2009. From January 2009 to October 2009, Mr. Renfro served as Executive Vice President of UnitedHealth Group and Chief Executive Officer of Ovations. Prior to joining UnitedHealth Group, Mr. Renfro served as President of Fidelity Developing Businesses at Fidelity Investments and as a member of the Fidelity Executive Committee from June 2008 to January 2009. From November 2005 to May 2008, Mr. Renfro held several senior positions at AARP Services Inc., including President and Chief Executive Officer of AARP Services Inc., Chief Operating Officer of AARP Services Inc., President and Chief Executive Officer of AARP Financial and President of the AARP Funds. From November 2004 to October 2005, Mr. Renfro served as Managing Director of Devonshire Financial Group. Mr. Renfro served as Chairman and Chief Executive Officer of New River Inc. from 1998 to October 2004.
Ms. Sweere is Executive Vice President of Human Capital of UnitedHealth Group and has served in that capacity since June 2007. Prior to joining UnitedHealth Group, Ms. Sweere served as Executive Vice President of Human Resources of CNA Corporation from October 2004 to April 2007 and held various leadership positions with CNA Corporation from 2003 to October 2004.
Mr. Walsh is Executive Vice President, General Counsel and Assistant Secretary of UnitedHealth Group and has served in that capacity since October 2009. From August 2007 to October 2009, Mr. Walsh served as Senior Vice President and Deputy General Counsel of UnitedHealth Group, and from January 2009 to October 2009,
13
Mr. Walsh served also as interim Co-Chief Legal Officer of UnitedHealth Group. Mr. Walsh joined UnitedHealth Group in August 2007. Prior to joining UnitedHealth Group, Mr. Walsh was a partner at Hogan and Hartson from July 2000 to August 2007.
Mr. Welters is Executive Vice President of UnitedHealth Group and President of the Public and Senior Market Group and has served in that capacity since September 2007. Mr. Welters was named Executive Vice President of UnitedHealth Group in November 2006. From 2004 to November 2006, Mr. Welters was President and Chief Executive Officer of AmeriChoice. Mr. Welters joined UnitedHealth Group in 2002 and held various executive positions with the Company from 2002 to 2004.
Mr. Wichmann is Executive Vice President of UnitedHealth Group and President of UnitedHealth Group Operations and has served in that capacity since April 2008. From December 2006 to April 2008, Mr. Wichmann served as Executive Vice President of UnitedHealth Group and President of the Commercial Markets Group (now UnitedHealthcare). From July 2004 to December 2006, Mr. Wichmann served as President and Chief Operating Officer of UnitedHealthcare. In 2004, Mr. Wichmann served as Chief Executive Officer of Specialized Care Services (now OptumHealth). Mr. Wichmann joined UnitedHealth Group in 1998 and held various executive positions with the Company from 1998 to 2004.
Mr. Zamoff is Executive Vice President, General Counsel and Assistant Secretary of UnitedHealth Group and has served in that capacity since October 2009. From March 2008 to October 2009, Mr. Zamoff served as General Counsel of UnitedHealthcare, and from January 2009 to October 2009, Mr. Zamoff served also as interim Co-Chief Legal Officer of UnitedHealth Group. Mr. Zamoff joined UnitedHealth Group in March 2008. Prior to joining UnitedHealth Group, Mr. Zamoff was a partner at Hogan and Hartson from January 2001 to March 2008, and from December 1996 to December 2000 Mr. Zamoff served as Assistant U.S. Attorney for the U.S. Department of Justice.
| ITEM 1A. | RISK FACTORS |
CAUTIONARY STATEMENTS
The statements, estimates, projections, guidance or outlook contained in this Annual Report on Form 10-K include forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 (PSLRA). When used in this Annual Report on Form 10-K and in future filings by us with the SEC, in our news releases, presentations to securities analysts or investors, and in oral statements made by or with the approval of one of our executive officers, the words or phrases "believe," "expect," "intend," "estimate," "anticipate," "plan," project," "should" or similar expressions are intended to identify such forward-looking statements. These statements are intended to take advantage of the "safe harbor" provisions of the PSLRA. These forward-looking statements involve risks and uncertainties that may cause our actual results to differ materially from the results discussed in the forward-looking statements.
The following discussion contains certain cautionary statements regarding our business that investors and others should consider. We do not undertake to address or update forward-looking statements in future filings or communications regarding our business or results of operations, and do not undertake to address how any of these factors may have caused results to differ from discussions or information contained in previous filings or communications. In addition, any of the matters discussed below may have affected past, as well as current, forward-looking statements about future results. Any or all forward-looking statements in this Form 10-K and in any other public filings or statements we make may turn out to be wrong. They can be affected by inaccurate assumptions we might make or by known or unknown risks and uncertainties. Many factors discussed below will be important in determining future results. By their nature, forward-looking statements are not guarantees of future performance or results and are subject to risks, uncertainties and assumptions that are difficult to predict or quantify. Actual future results may vary materially from expectations expressed in this report or any of our prior communications.
14
Proposed health care reforms could materially adversely affect our revenues, financial position and our results of operations.
Both houses of Congress have recently passed bills relating to health care reform, which have not yet been reconciled with each other and signed into law. Examples of health care reform proposals include policy changes that would change the dynamics of the health care industry, including having the federal or one or more state governments assume a larger role in the health care system such as competing with private health insurers, imposing new and potentially significant taxes on health insurers and health care benefits, guaranteed coverage requirements, elimination of pre-existing condition exclusions or annual lifetime maximum limits, restrictions on our ability to price products based on our underwriting standards, or restructuring the Medicare or Medicaid programs, including reducing payments to private plans offering Medicare Advantage over the intermediate term. In addition, from time to time, Congress has considered various forms of managed care reform legislation, which, if adopted, could fundamentally alter the treatment of coverage decisions under ERISA. Additionally, there is legislative interest in modifying ERISA's preemptive effect on state laws. If adopted, such limitations could increase our liability exposure and could permit greater state regulation of our operations.
A number of state legislatures, including California, Colorado, New York, Ohio and Pennsylvania, have contemplated but have not enacted significant reform of their health insurance markets. Other states are expected to consider significant reform of their health insurance markets as well as more modest reforms aimed at expanding Medicaid and/or SCHIP eligibility and new coverage options for those not eligible for government programs. These proposals include provisions affecting both public programs and privately financed health insurance arrangements. States also are considering proposals that would reform the underwriting and marketing practices of individual and group health insurance products by, for example, placing restrictions on rating and pricing and mandating minimum medical benefit cost ratios.
The enactment of health care reforms at the federal or state level may affect certain aspects of our business, including contracting with physicians, hospitals and/or other health care professionals; medical, administrative, technology or other costs; physician reimbursement methods and payment rates; premium rates; coverage determinations; mandated benefits; minimum medical expenditures; claim payments and processing; drug utilization and patient safety efforts; collection, use, disclosure, maintenance and disposal of individually identifiable health information; personal health records; consumer-driven health plans and health savings accounts and insurance market reforms; and government-sponsored programs.
We cannot predict if any of these proposals will ultimately become law, or, if enacted, what their terms or the regulations promulgated pursuant to such laws will be. Any health care reforms enacted may be phased in over a number of years but, if enacted, could reduce our revenues, increase our costs, expose us to expanded liability and require us to revise the ways in which we conduct business or put us at risk for loss of business. In addition, our results of operations, our financial position, including our ability to maintain the value of our goodwill, and cash flows could be materially adversely affected by such changes.
If we fail to effectively estimate, price for and manage our medical costs, the profitability of our risk-based products could decline and could materially adversely affect our future financial results.
Under our risk-based product arrangements, we assume the risk of both medical and administrative costs for our customers in return for monthly premiums. Premium revenues from risk-based products comprise approximately 90% of our total consolidated revenues. We generally use approximately 80% to 85% of our premium revenues to pay the costs of health care services delivered to these customers. The profitability of our risk-based products depends in large part on our ability to predict, price for, and effectively manage medical costs.
We manage medical costs through underwriting criteria, product design, negotiation of favorable provider contracts and care management programs. Total medical costs are affected by the number of individual services rendered and the cost of each service. Our premium revenue on commercial policies is typically fixed for a
15
12-month period and is generally priced one to four months before the contract commences. Our revenue on Medicare policies is based on bids submitted in June the year before the contract year. We base the premiums we charge and our Medicare bids on our estimates of future medical costs over the fixed contract period; however, medical cost inflation, regulation and other factors may cause actual costs to exceed what was estimated and reflected in premiums or bids. These factors may include increased use of services, increased cost of individual services, catastrophes, epidemics, the introduction of new or costly treatments and technology, new mandated benefits or other regulatory changes, insured population characteristics and seasonal changes in the level of health care use. As a measure of the impact of medical costs on our financial results, relatively small differences between predicted and actual medical costs or utilization rates as a percentage of revenues can result in significant changes in our financial results. For example, if medical costs increased by 1% without a proportional change in related revenues for commercial insured products, our annual net earnings for 2009 would have been reduced by approximately $200 million.
In addition, the financial results we report for any particular period include estimates of costs that have been incurred for which claims are still outstanding. These estimates involve an extensive degree of judgment. If these estimates prove too low, they will have a negative impact on our future results.
Our business activities are highly regulated; new laws or regulations or changes in existing laws or regulations or their enforcement could materially adversely affect our results of operations, financial position and cash flows.
Our business is regulated at the federal, state, local and international levels. The laws and rules governing our business and interpretations of those laws and rules are subject to frequent change. For example, in 2009, CMS implemented a reduction in Medicare Advantage reimbursements of approximately 5% for 2010. Although we have adjusted members' benefits and premiums on a selective basis, terminated benefit plans in certain counties, and intensified both our medical and operating cost management in response to these rate reductions, there can be no assurance that we will be able to execute successfully on these or other strategies to address changes in the Medicare Advantage program. Our results of operations, financial position and cash flows could be materially adversely affected by such reductions.
The broad latitude that is given to the agencies administering regulations governing our business, as well as future laws and rules, could force us to change how we do business, restrict revenue and enrollment growth, increase our health care and administrative costs and capital requirements, and increase our liability in federal and state courts for coverage determinations, contract interpretation and other actions. For example, in October 2008 Congress enacted the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA), which requires insurers to provide mental health and substance use disorder benefits under terms that are no more restrictive than those applied to medical and surgical benefits. The MHPAEA specifically directed the Secretaries of Labor, Health and Human Services and the Treasury to issue regulations to effectuate the legislation. Although regulations regarding how the MHPAEA will be implemented were issued on February 2, 2010 in the form of an interim final rule, final regulations have not yet been published. Because of the broad range of treatment limitations to which parity is expected to apply under the regulations, the regulations will likely lead to an increase in the costs associated with both insured and self-insured plans for behavioral health benefits and services and impact our market for carve-out health benefit administration, which could have an adverse effect on our earnings from operations.
We must also obtain and maintain regulatory approvals to market many of our products, to increase prices for certain regulated products and to complete certain acquisitions and dispositions, including integration of certain acquisitions. Delays in obtaining approvals or our failure to obtain or maintain these approvals could reduce our revenue or increase our costs.
In August 2007, we entered into a multi-state national agreement with regulatory offices in 39 states and the District of Columbia relating to UnitedHealthcare's fully insured commercial business administered on the
16
organization's main processing platforms. The agreement covers several key areas of review of our business operations, including claims payment accuracy and timeliness, appeals and grievances resolution timeliness, health care professional network/service, utilization review, explanation of benefits accuracy, and oversight and due diligence of contracted entities and vendor performance. The agreement addressed and resolved past regulatory matters related to the areas of review prior to August 2007 and establishes a transparent framework for evaluating and regulating performance through December 2010. The agreement is similar to a customer performance guarantee, whereby we self report quarterly and annually our current operational performance on a set of national performance standards agreed to by the participating states. We must perform to the standards set forth in the agreement, or be subject to fines and penalties.
We are also involved in various governmental investigations, audits and reviews. These regulatory activities include routine, regular and special investigations, audits and reviews by CMS, state insurance and health and welfare departments and state attorneys general, the Office of the Inspector General, the Office of Personnel Management, the Office of Civil Rights, U.S. Congressional committees, the U.S. Department of Justice, U.S. Attorneys, the SEC, the IRS, the U.S. Department of Labor and other governmental authorities. For example, in 2007, the California Department of Insurance examined our PacifiCare health insurance plan in California. The examination findings related to claims processing accuracy and timeliness, accurate and timely interest payments, timely implementation of provider contracts, timely, accurate provider dispute resolution, and other related matters. The matter is now the subject of an administrative proceeding before an administrative law judge. In addition, the U.S. Department of Labor is conducting an investigation of our administration of our employee benefit plans with respect to ERISA compliance. Reviews and investigations of this sort can lead to government actions, which can result in the assessment of damages, civil or criminal fines or penalties, or other sanctions, including restrictions or changes in the way we conduct business, loss of licensure or exclusion from participation in government programs, and could have a material adverse effect on our business and results of operations.
In addition, the health care industry is subject to negative publicity. Negative publicity, including negative publicity surrounding routine governmental investigations, may adversely affect our stock price, damage our reputation in various markets and result in increased regulation and legislative review of industry practices, which may further increase our costs of doing business and adversely affect our profitability by adversely affecting our ability to market our products and services, requiring us to change our products and services, or increasing the regulatory burdens under which we operate.
For a discussion of various federal and state laws and regulations governing our businesses, see Item 1, "Business – Government Regulation."
Adverse economic conditions could adversely affect our revenues and our results of operations.
The current recessionary U.S. economic environment may continue to impact demand for certain of our products and services. For example, higher unemployment rates and significant employment layoffs and downsizings have caused and could continue to lead to lower enrollment in our employer group plans, lower enrollment in our non-employer individual plans and a higher number of employees opting out of our employer group plans. Adverse economic conditions have caused and could continue to cause employers to stop offering certain health care coverage as an employee benefit or elect to offer this coverage on a voluntary, employee-funded basis as a means to reduce their operating costs. In addition, the economic downturn could continue to negatively impact our employer group renewal prospects and our ability to increase premiums and could result in cancellation of products and services by our customers. All of these could lead to a decrease in our membership levels and premium and fee revenues and could adversely affect our results of operations. In addition, a prolonged economic downturn could negatively impact the financial position of hospitals and other care providers and therefore could adversely affect our contracted rates with these parties and increase our medical costs.
17
During a prolonged economic downturn, state and federal budgets could be adversely affected, resulting in reduced reimbursements or payments in our federal and state government health care coverage programs, including Medicare, Medicaid and SCHIP. A reduction in state Medicaid reimbursement rates could be implemented retrospectively to payments already negotiated and/or received from the government and could adversely affect our revenues and results of operations. In addition, the state and federal budgetary pressures could cause the government to impose new or a higher level of taxes or assessments for our commercial programs, such as premium taxes on insurance companies and health maintenance organizations and surcharges on select fee-for-service and capitated medical claims, and could adversely affect our results of operations.
Our businesses providing PBM services face regulatory and other risks and uncertainties associated with the PBM industry that may differ from the risks of our business of providing managed care and health insurance products.
We provide PBM services through our Prescription Solutions and UnitedHealthcare businesses. Each business is subject to federal and state anti-kickback and other laws that govern their relationships with pharmaceutical manufacturers, customers and consumers. In addition, federal and state legislatures regularly consider new regulations for the industry that could adversely affect current industry practices, including the receipt or required disclosure of rebates from pharmaceutical companies. See Item 1, "Business – Government Regulation" for a discussion of various federal and state laws and regulations governing our PBM businesses.
Our PBM businesses provide services to sponsors of health benefit plans that are subject to ERISA. The DOL, which is the agency that enforces ERISA, could assert that the fiduciary obligations imposed by the statute apply to some or all of the services provided by our PBM businesses even where our PBM businesses are not contractually obligated to assume fiduciary obligations. In the event a court were to determine that fiduciary obligations apply to our PBM businesses in connection with services for which our PBM businesses are not contractually obligated to assume fiduciary obligations, we could be subject to claims for breaches of fiduciary obligations or entering into certain prohibited transactions.
Prescription Solutions also conducts business as a mail order pharmacy, which subjects it to extensive federal, state and local laws and regulations. The failure to adhere to these laws and regulations could expose Prescription Solutions to civil and criminal penalties. Further, Prescription Solutions is subject to the Payment Card Industry Data Security Standards, which is a multifaceted security standard that includes requirements for security management, policies, procedures, network architecture, software design and other critical protective measures to protect customer account data as mandated by the credit card brands. The failure to adhere to such standards could expose Prescription Solutions to liability or impact their ability to process credit card transactions.
In addition, our PBM businesses would be adversely affected by an inability to contract on favorable terms with pharmaceutical manufacturers and could face potential claims in connection with purported errors by our mail order pharmacies, including in connection with the risks inherent in the packaging and distribution of pharmaceuticals and other health care products. Disruptions at any of our mail order pharmacies due to failure of technology or any other failure or disruption to these systems or to the infrastructure due to fire, electrical outage, natural disaster, acts of terrorism or some other catastrophic event could reduce our ability to process and dispense prescriptions and provide products and services to customers.
If we fail to compete effectively to maintain or increase our market share, including maintaining or increasing enrollments in businesses providing health benefits, our results of operations could be materially adversely affected.
Our businesses compete throughout the United States and face competition in all of the geographic markets in which we operate. We compete with other companies on the basis of many factors, including price of benefits offered and cost and risk of alternatives, location and choice of health care providers, quality of customer service,
18
comprehensiveness of coverage offered, reputation for quality care, financial stability and diversity of product offerings. For our Health Benefits reporting segment, competitors include Aetna Inc., Cigna Corporation, Coventry Health Care, Inc., Health Net, Inc., Humana Inc., Kaiser Permanente, WellPoint, Inc., numerous for-profit and not-for-profit organizations operating under licenses from the Blue Cross Blue Shield Association and other enterprises that serve more limited geographic areas or market segments such as Medicare specialty services. For our Prescription Solutions business, competitors include Medco Health Solutions, Inc., CVS/Caremark Corporation and Express Scripts, Inc. Our OptumHealth and Ingenix reporting segments also compete with a broad and diverse set of other businesses.
We believe that barriers to entry in many markets are not substantial, so the addition of new competitors can occur relatively easily, and customers enjoy significant flexibility in moving between competitors. In particular markets, competitors may have capabilities or resources that give them a competitive advantage. Greater market share, established reputation, superior supplier or health care professional arrangements, existing business relationships, and other factors all can provide a competitive advantage to our businesses or to their competitors.
In addition, significant merger and acquisition activity has occurred in the industries in which we operate, both as to our competitors and suppliers (including hospitals, physician groups and other care professionals) in these industries. Consolidation may make it more difficult for us to retain or increase customers, to improve the terms on which we do business with our suppliers, or to maintain or advance profitability. If we do not compete effectively in our markets, if we set rates too high or too low in highly competitive markets, if we do not design and price our products properly and competitively, if we are unable to innovate and deliver products and services that demonstrate value to our customers, if we do not provide a satisfactory level of services, if membership or demand for other services does not increase as we expect, if membership or demand for other services declines, or if we lose accounts with more profitable products while retaining or increasing membership in accounts with less profitable products, our business and results of operations could be materially adversely affected.
As a payer in various government health care programs, we are exposed to additional risks associated with program funding, enrollments, payment adjustments and audits that could adversely affect our revenues, cash flows and results of operations.
We participate in various federal, state and local government health care coverage programs, including as a payer in Medicare Advantage, Medicare Part D, various Medicaid programs and SCHIP, and receive revenues from these programs. These programs generally are subject to frequent changes, including changes that may reduce the number of persons enrolled or eligible, reduce the amount of reimbursement or payment levels, or increase our administrative or medical costs under such programs. For example, CMS recently implemented a reduction in Medicare Advantage reimbursements of approximately 5% for 2010. Such changes have adversely affected our results of operations and willingness to participate in such programs in certain geographic areas in the past, and may do so in the future.
Our participation in the Medicare Advantage, Medicare Part D, and various Medicaid programs and SCHIP occurs through bids that are submitted periodically. Revenues for these programs are dependent upon periodic funding from the federal government or applicable state governments and allocation of the funding through various payment mechanisms. Funding for these government programs is dependent upon many factors outside of our control, including general economic conditions and budgetary constraints at the federal or applicable state level, and general political issues and priorities. A reduction or less than expected increase in government funding for these programs or change in allocation methodologies may adversely affect our revenues and results of operations.
CMS uses various payment mechanisms to allocate funding for Medicare programs, including determining payments by considering the risk status of our Medicare members as supported by provider medical record documentation. Federal regulators audit the supporting documents and can revise payments based on the audit findings. CMS announced in 2008 that it will perform audits of selected Medicare health plans each year to
19
validate the coding practices of and supporting documentation maintained by care providers. These audits involve a review of medical records maintained by providers, including those in and out of network, and may result in prospective and retrospective adjustments to payments made to health plans pursuant to CMS Medicare contracts. Certain of our plans have been selected for audit. The first audits focused on medical records supporting risk adjustment data for 2006 that were used to determine 2007 payment amounts. The Office of Inspector General for HHS is conducting an audit of our risk adjustment data for two plans. We are unable to predict the outcome of the audits. However, any material adjustments could have a material effect on our results of operations.
Our ability to retain and acquire Medicare, Medicaid and SCHIP enrollees is impacted by bids and plan designs submitted by our competitors and us. Under the Medicaid Managed Care program, state Medicaid agencies are periodically required by federal law to seek bids from eligible health plans to continue their participation in the acute care Medicaid health programs. If we are not successful in obtaining renewals of state Medicaid Managed Care contracts, we risk losing the members that were enrolled in those Medicaid plans. Under the Medicare Part D program, to qualify for automatic enrollment of low income members, our bids must result in an enrollee premium below a threshold, which is set by the government after our bids are submitted. If the enrollee premium is not below the government threshold, we risk losing the members who were auto-assigned to us and we will not have additional members auto-assigned to us. For example, we lost approximately 650,000 of our auto-enrolled low-income subsidy members in 2008 because certain of our bids exceeded thresholds set by the government. In general, our bids are based upon certain assumptions regarding enrollment, utilization, medical costs, and other factors. In the event any of these assumptions are materially incorrect or our competitors' bids and positioning are different than anticipated, either as a result of unforeseen changes to the Medicare program or otherwise, our results of operations could be materially affected.
If we fail to develop and maintain satisfactory relationships with physicians, hospitals, and other health care providers, our business could be adversely affected.
We contract with physicians, hospitals, pharmaceutical benefit service providers, pharmaceutical manufacturers, and other health care providers for competitive prices and services. Our results of operations and prospects are substantially dependent on our continued ability to maintain these competitive prices and services. Failure to develop and maintain satisfactory relationships with health care providers, whether in-network or out-of-network, could adversely affect our business and results of operations.
In any particular market, physicians and health care providers could refuse to contract, demand higher payments, or take other actions that could result in higher medical costs, less desirable products for customers or difficulty meeting regulatory or accreditation requirements. In some markets, certain health care providers, particularly hospitals, physician/hospital organizations or multi-specialty physician groups, may have significant market positions or near monopolies that could result in diminished bargaining power on our part. In addition, physician or practice management companies, which aggregate physician practices for administrative efficiency and marketing leverage, may compete directly with us. If these providers refuse to contract with us, use their market position to negotiate favorable contracts or place us at a competitive disadvantage, our ability to market products or to be profitable in those areas could be adversely affected.
In addition, we have capitation arrangements with some physicians, hospitals and other health care providers. Under the typical arrangement, the health care provider receives a fixed percentage of premium to cover all or a defined portion of the medical costs provided to the capitated member. Under some capitated arrangements, the provider may also receive additional compensation from risk sharing and other incentive arrangements. Capitation arrangements limit our exposure to the risk of increasing medical costs, but expose us to risk related to the adequacy of the financial and medical care resources of the professional. To the extent that a capitated health care provider organization faces financial difficulties or otherwise is unable to perform its obligations under the capitation arrangement, we may be held responsible for unpaid health care claims that should have been the responsibility of the capitated health care provider and for which we have already paid the provider under the capitation arrangement. Further, payment or other disputes between a primary care provider and specialists with
20
whom the primary care provider contracts can result in a disruption in the provision of services to our members or a reduction in the services available to our members. There can be no assurance that health care providers with whom we contract will properly manage the costs of services, maintain financial solvency or avoid disputes with other providers. Any of these events could have an adverse effect on the provision of services to our members and our operations.
In addition, some providers that render services to our members do not have contracts with us. In those cases, we do not have a pre-established understanding with the provider about the amount of compensation that is due to the provider for services rendered to our members. In some states, the amount of compensation due to these out-of-network providers is defined by law or regulation, but in most instances, it is either not defined or it is established by a standard that is not clearly translatable into dollar terms. In some instances, providers may believe that they are underpaid for their services and may either litigate or arbitrate their dispute with us or try to recover from our members the difference between what we have paid them and the amount they charged us. For example, we are involved in litigation with out-of-network providers that is described in more detail in "Legal Matters" in Note 14 of Notes to the Consolidated Financial Statements. Failure to maintain satisfactory relationships with out-of-network health care providers could adversely affect our business and results of operations.
Sales of our products and services are dependent on our ability to attract, retain and provide support to a network of independent third party brokers, consultants and agents.
Our products are sold in part through independent brokers, consultants and agents who assist in the production and servicing of business. We typically do not have long-term contracts with our independent brokers, consultants and agents, who generally are not exclusive to us and who typically also recommend and/or market health care products and services of our competitors. As a result, we must compete intensely for their services and allegiance. Our sales would be adversely affected if we are unable to attract or retain independent brokers, consultants and agents or if we do not adequately provide support, training and education to them regarding our product portfolio, which is complex, or if our sales strategy is not appropriately aligned across distribution channels.
In addition, there have been a number of investigations regarding the marketing practices of brokers and agents selling health care products and the payments they receive. These have resulted in enforcement actions against companies in our industry and brokers and agents marketing and selling these companies' products. For example, CMS and state departments of insurance have increased their scrutiny of the marketing practices of brokers and agents who market Medicare products. These investigations and enforcement actions could result in penalties and the imposition of corrective action plans and/or changes to industry practice, which could adversely impact our ability to market our products.
If we fail to comply with restrictions on patient privacy and data security regulations, including taking steps to ensure that our business associates who obtain access to sensitive patient information maintain its confidentiality and security, our reputation and business operations could be materially adversely affected.
The collection, maintenance, protection, use, transmission, disclosure and disposal of individually identifiable data by our businesses are regulated at the international, federal and state levels. These laws and rules are subject to change by legislation or administrative or judicial interpretation. Various state laws address the use and disclosure of individually identifiable health information to the extent they are more restrictive than those contained in the privacy and security provisions in the federal GLBA and in HIPAA. HIPAA now requires business associates as well as covered entities to comply with certain privacy and security requirements. See Item 1, "Business – Government Regulation" for a discussion of various federal and state privacy laws and regulations governing our businesses.
Even though we provide for appropriate protections through our contracts with our business associates and in certain cases assess our business associates' security controls, we still have limited control over their actions and
21
practices. Privacy and security requirements regarding personally identifiable information are also imposed on us through controls with our customers. In addition, despite the security measures we have in place to ensure compliance with applicable laws and rules, our facilities and systems and those of our third party service providers may be vulnerable to security breaches, acts of vandalism or theft, computer viruses, misplaced or lost data, programming and/or human errors or other similar events. Compliance with new privacy and security laws, requirements, and new regulations, such as ARRA, will result in cost increases due to necessary systems changes (including further implementation of encryption and other data protection standards), new limitations or constraints on our business models, the development of new administrative processes, the effects of potential noncompliance by our business associates, and increased enforcement actions and fines and penalties. They also may impose further restrictions on our collection, disclosure and use of patient identifiable data that is housed in one or more of our administrative databases.
Noncompliance with any privacy or security laws and regulations or any security breach involving the misappropriation, loss or other unauthorized disclosure of sensitive or confidential member information, whether by us or by one of our business associates, could have a material adverse effect on our business, reputation and results of operations, including mandatory disclosure to the media, significant increase in the number and cost of managing and remediating data security incidents, increased enforcement actions, material fines and penalties, compensatory, special, punitive, and statutory damages, litigation, consent orders regarding our privacy and security practices, adverse actions against our licenses to do business, and injunctive relief.
Our relationship with AARP is important and the loss of such relationship could have an adverse effect on our business and results of operations.
Under our agreements with AARP, we provide AARP-branded Medicare Supplement insurance, hospital indemnity insurance and other products to AARP members and Medicare Part D prescription drug plans to AARP members and non-members. One of our agreements with AARP expands the relationship to include AARP-branded Medicare Advantage plans for AARP members and non-members. Our agreements with AARP contain commitments regarding corporate governance, corporate social responsibility, diversity and measures intended to improve and simplify the health care experience for consumers. The AARP agreements may be terminated early under certain circumstances, including, depending on the agreement, a material breach by either party, insolvency of either party, a material adverse change in the financial condition of the Company, material changes in the Medicare programs, material harm to AARP caused by the Company, and by mutual agreement. The success of our AARP arrangements depends, in part, on our ability to service AARP and its members, develop additional products and services, price the products and services competitively, meet our corporate governance, corporate social responsibility, and diversity commitments, and respond effectively to federal and state regulatory changes. The loss of our AARP relationship could have an adverse effect on our business and results of operations.
Because of the nature of our business, we are routinely subject to various litigation actions, which, if resolved unfavorably, could result in substantial penalties and/or monetary damages and adversely affect our financial position, results of operations and cash flows.
Periodically, we become a party to the types of legal actions that can affect any business, such as employment and employment discrimination-related suits, employee benefit claims, breach of contract actions, tort claims, shareholder suits, and intellectual property-related litigation. In addition, because of the nature of our business, we are routinely made party to a variety of legal actions related to the design and management of our service offerings. These matters include, among others, claims related to health care benefits coverage and payment (including disputes with enrollees, customers, and contracted and non-contracted physicians, hospitals and other health care professionals), tort, contract disputes and claims related to disclosure of certain business practices. We are also party to certain class action lawsuits brought by health care professional groups.
We are largely self-insured with regard to litigation risks. Although we maintain excess liability insurance with outside insurance carriers for claims in excess of our self-insurance, certain types of damages, such as punitive
22
damages in some circumstances, are not covered by insurance. We record liabilities for our estimates of the probable costs resulting from self-insured matters; however, it is possible that the level of actual losses will exceed the liabilities recorded.
A description of significant legal actions in which we are currently involved is included in Note 14 of Notes to the Consolidated Financial Statements. We cannot predict the outcome of these actions with certainty, and we are incurring expenses in resolving these matters. Therefore, these legal actions could further increase our cost of doing business and adversely affect our financial position, results of operations and cash flows.
Our investment portfolio may suffer losses, which could materially adversely affect our results of operations.
Fluctuations in the fixed income or equity markets could impair our profitability and capital position. Volatility in interest rates affects our interest income and the market value of our investments in debt securities of varying maturities, which comprise the vast majority of the fair value of our investments as of December 31, 2009. In addition, defaults by issuers, primarily from investments in liquid corporate and municipal bonds, who fail to pay or perform on their obligations, could reduce our investment income and net realized investment gains or result in net realized investment losses as we may be required to write down the value of our investments, which would adversely affect our profitability and shareholders' equity.
We also invest a small proportion of our investments in equity investments, which are subject to greater volatility than fixed income investments. General economic conditions, stock market conditions, and many other factors beyond our control can adversely affect the value of our equity investments and may result in investment losses.
There can be no assurance that our investments will produce total positive returns or that we will not sell investments at prices that are less than the carrying value of these investments. Changes in the value of our investment assets, as a result of interest rate fluctuations, illiquidity or otherwise, could have a negative effect on our shareholders' equity. In addition, if it became necessary for us to liquidate our investment portfolio on an accelerated basis, it could have an adverse effect on our results of operations.
If the value of our intangible assets is materially impaired, our results of operations, shareholders' equity and debt ratings could be materially adversely affected.
Goodwill and other intangible assets were $23.1 billion as of December 31, 2009, representing 39% of our total assets. We periodically evaluate our goodwill and other intangible assets to determine whether all or a portion of their carrying values may be impaired, in which case a charge to earnings may be necessary. For example, the enactment of health care reforms may impact our ability to maintain the value of our goodwill and other intangible assets in some of our businesses, as any passed legislation may significantly change the growth rate assumptions for some of our businesses. Any future evaluations requiring an impairment of our goodwill and other intangible assets could materially affect our results of operations and shareholders' equity in the period in which the impairment occurs. A material decrease in shareholders' equity could, in turn, negatively impact our debt ratings or potentially impact our compliance with existing debt covenants.
Large-scale medical emergencies may result in significant medical costs and may have a material adverse effect on our business, financial condition and results of operations.
Large-scale medical emergencies can take many forms and can cause widespread illness and death. Such emergencies could materially and adversely affect the U.S. economy in general and the health care industry specifically. For example, in the event of a natural disaster, bioterrorism attack, pandemic or other extreme events, we could face, among other things, significant medical costs and increased use of health care services. Any such disaster or similar event could have a material adverse effect on our business, financial condition and results of operations.
23
If we fail to properly maintain the integrity or availability of our data or to strategically implement new or upgrade or consolidate existing information systems, our business could be materially adversely affected.
Our ability to adequately price our products and services, to provide effective service to our customers in an efficient and uninterrupted fashion, and to accurately report our results of operations depends on the integrity of the data in our information systems. As a result of technology initiatives and recently enacted regulations, changes in our system platforms and integration of new business acquisitions, we have been taking steps to consolidate and integrate the number of systems we operate and have upgraded and expanded our information systems capabilities. Our information systems require an ongoing commitment of significant resources to maintain, protect and enhance existing systems and develop new systems to keep pace with continuing changes in information processing technology, evolving systems and regulatory standards, and changing customer patterns. If the information we rely upon to run our businesses were found to be inaccurate or unreliable or if we fail to maintain or protect our information systems and data integrity effectively, we could lose existing customers, have difficulty attracting new customers, have problems in determining medical cost estimates and establishing appropriate pricing, have difficulty preventing, detecting and controlling fraud, have disputes with customers, physicians and other health care professionals, have regulatory sanctions or penalties imposed, have increases in operating expenses or suffer other adverse consequences. There can be no assurance that our process of consolidating the number of systems we operate, upgrading and expanding our information systems capabilities, protecting and enhancing our systems and developing new systems to keep pace with continuing changes in information processing technology will be successful or that additional systems issues will not arise in the future. Failure to consolidate and integrate our systems successfully could result in higher than expected costs and diversion of management's time and energy, which could materially impact our business, financial condition and results of operations.
If we are not able to protect our proprietary rights to our databases and related products, our ability to market our knowledge and information-related businesses could be hindered and our business could be adversely affected.
We rely on our agreements with customers, confidentiality agreements with employees, and our trademarks, trade secrets, copyrights and patents to protect our proprietary rights. These legal protections and precautions may not prevent misappropriation of our proprietary information. In addition, substantial litigation regarding intellectual property rights exists in the software industry, and we expect software products to be increasingly subject to third-party infringement claims as the number of products and competitors in this industry segment grows. Such litigation and misappropriation of our proprietary information could hinder our ability to market and sell products and services and our revenues and results of operations could be adversely affected.
Our ability to obtain funds from some of our subsidiaries is restricted and if we are unable to obtain sufficient funds from our subsidiaries to fund our obligations, our operations or financial position may be adversely affected.
Because we operate as a holding company, we are dependent upon dividends and administrative expense reimbursements from some of our subsidiaries to fund our obligations. These subsidiaries generally are regulated by states' departments of insurance. We are also required by law to maintain specific prescribed minimum amounts of capital in these subsidiaries. The levels of capitalization required depend primarily upon the volume of premium revenues generated. A significant increase in premium volume will require additional capitalization from us. In most states, we are required to seek prior approval by these state regulatory authorities before we transfer money or pay dividends from these subsidiaries that exceed specified amounts. In addition, we normally notify the state departments of insurance prior to making payments that do not require approval. An inability of our regulated subsidiaries to pay dividends to their parent companies could impact the scale to which we could reinvest in our business through capital expenditures, business acquisitions and the repurchase of shares of our common stock and our ability to repay our debt. If we are unable to obtain sufficient funds from our subsidiaries to fund our obligations, our operations or financial position may be adversely affected.
24
Any failure by us to manage and complete acquisitions and other significant transactions successfully could harm our results of operations, business and prospects.
As part of our business strategy, we frequently engage in discussions with third parties regarding possible investments, acquisitions, divestitures, strategic alliances, joint ventures, and outsourcing transactions and often enter into agreements relating to such transactions. If we fail to identify and complete successfully transactions that further our strategic objectives, we may be required to expend resources to develop products and technology internally, we may be at a competitive disadvantage or we may be adversely affected by negative market perceptions, any of which may have a material adverse effect on our results of operations, financial position or cash flows. For acquisitions, success is also dependent upon efficiently integrating the acquired business into our existing operations. If we are unable to successfully integrate and grow these acquisitions and to realize contemplated revenue synergies and cost savings, our results of operations could be adversely affected.
Downgrades in our credit ratings, should they occur, may adversely affect our business, financial condition and results of operations.
Claims paying ability, financial strength, and credit ratings by recognized rating organizations are important factors in establishing the competitive position of insurance companies. Ratings information is broadly disseminated and generally used throughout the industry. We believe our claims paying ability and financial strength ratings are important factors in marketing our products to certain of our customers. Our debt ratings impact both the cost and availability of future borrowings. Each of the rating agencies reviews its ratings periodically and there can be no assurance that current ratings will be maintained in the future. Our ratings reflect each rating agency's opinion of our financial strength, operating performance and ability to meet our debt obligations or obligations to policyholders. Downgrades in our credit ratings, should they occur, may adversely affect our business, financial condition and results of operations.
| ITEM 1B. | UNRESOLVED STAFF COMMENTS |
None.
| ITEM 2. | PROPERTIES |
As of December 31, 2009, we owned and/or leased real properties totaling approximately 15.2 million square feet to support our business operations in the United States and other countries. Our facilities are primarily located in the United States. Of this total, we owned approximately 1 million aggregate square feet of space and leased the remainder. Our leases expire at various dates through September 30, 2028. Our various reporting segments use these facilities for their respective business purposes, and we believe these current facilities are suitable for their respective uses and are adequate for our anticipated future needs.
| ITEM 3. | LEGAL PROCEEDINGS |
See Note 14 of Notes to the Consolidated Financial Statements in this Form 10-K, which is incorporated by reference herein.
| ITEM 4. | SUBMISSION OF MATTERS TO A VOTE OF SECURITY HOLDERS |
None.
25
PART II
| ITEM 5. | MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
MARKET PRICES
Our common stock is traded on the New York Stock Exchange (NYSE) under the symbol UNH. On February 3, 2010, there were 18,145 registered holders of record of our common stock. The per share high and low common stock sales prices reported by the NYSE were as follows:
| High | Low | |||||
2010 | ||||||
First quarter (through February 3, 2010) | $ | 36.07 | $ | 30.97 | ||
2009 | ||||||
First quarter | $ | 30.25 | $ | 16.18 | ||
Second quarter | $ | 29.69 | $ | 19.85 | ||
Third quarter | $ | 30.00 | $ | 23.69 | ||
Fourth quarter | $ | 33.25 | $ | 23.50 | ||
2008 | ||||||
First quarter | $ | 57.86 | $ | 33.57 | ||
Second quarter | $ | 38.33 | $ | 25.50 | ||
Third quarter | $ | 33.49 | $ | 21.00 | ||
Fourth quarter | $ | 27.31 | $ | 14.51 | ||
DIVIDEND POLICY
Our Board of Directors established our dividend policy in August 1990. Pursuant to our dividend policy, our Board of Directors reviews our consolidated financial statements following the end of each fiscal year and decides whether to declare a dividend on the outstanding shares of common stock. On February 9, 2010, our Board of Directors approved an annual dividend of $0.03 per share, which will be paid on April 20, 2010 to shareholders of record on April 6, 2010. Shareholders of record on April 2, 2009 received an annual dividend for 2009 of $0.03 per share and shareholders of record on April 2, 2008 received an annual dividend for 2008 of $0.03 per share.
ISSUER PURCHASES OF EQUITY SECURITIES
Issuer Purchases of Equity Securities (a)
Fourth Quarter 2009
For the Month Ended | Total Number of Shares Purchased | Average Price Paid per Share | Total Number of Shares Purchased as Part of Publicly Announced Plans or Programs | Maximum Number of Shares That May Yet Be Purchased Under The Plans or Programs(a) | ||||||
October 31, 2009 | 880,797 | (b) | $ | 25.04 | 878,313 | 35,583,125 | ||||
November 30, 2009 | 709,550 | $ | 28.18 | 709,550 | 34,873,575 | |||||
December 31, 2009 | 6,274,229 | (c) | $ | 30.76 | 6,216,220 | 28,657,355 | ||||
TOTAL | 7,864,576 | $ | 29.88 | 7,804,083 | ||||||
| (a) | In November 1997, our Board of Directors adopted a share repurchase program, which the Board evaluates periodically. In February 2010, the Board renewed and increased our share repurchase program, and authorized us to repurchase up to 120 million shares of our common stock at prevailing market prices. There is no established expiration date for the program. The maximum number of shares that may be purchased under the plans or programs as of December 31, 2009 does not reflect this increase. |
26
| (b) | Represents 878,313 shares of our common stock repurchased during the period, and 2,484 shares of our common stock withheld by us, as permitted by the applicable equity award certificates, to satisfy tax withholding obligations upon vesting of shares of restricted stock. |
| (c) | Represents 6,216,220 shares of our common stock repurchased during the period, and 58,009 shares of our common stock withheld by us, as permitted by the applicable equity award certificates, to satisfy tax withholding obligations upon vesting of shares of restricted stock. |
PERFORMANCE GRAPHS
The following two performance graphs compare the Company's total return to shareholders with indexes of other specified companies and the S&P 500 Index. The first graph compares the cumulative five-year total return to shareholders on UnitedHealth Group's common stock relative to the cumulative total returns of the S&P 500 index and a customized peer group (the " Fortune 50 Group"), an index of certain Fortune 50 companies for the five-year period ended December 31, 2009. The second graph compares our cumulative total return to shareholders with the S&P 500 Index and an index of a group of peer companies selected by us for the five-year period ended December 31, 2009. The Company is not included in either the Fortune 50 Group index in the first graph or the peer group index in the second graph. In calculating the cumulative total shareholder return of the indexes, the shareholder returns of the Fortune 50 Group companies in the first graph and the peer group companies in the second graph are weighted according to the stock market capitalizations of the companies at January 1 of each year. The comparisons assume the investment of $100 on December 31, 2004 in Company common stock and in each index, and that dividends were reinvested when paid.
27
Fortune 50 Group
The Fortune 50 Group consists of the following companies: American International Group, Inc., Berkshire Hathaway Inc., Cardinal Health, Inc., Citigroup Inc., General Electric Company, International Business Machines Corporation and Johnson & Johnson. Although there are differences in terms of size and industry, like UnitedHealth Group, all of these companies are large multi-segment companies using a well-defined operating model in one or more broad sectors of the economy.
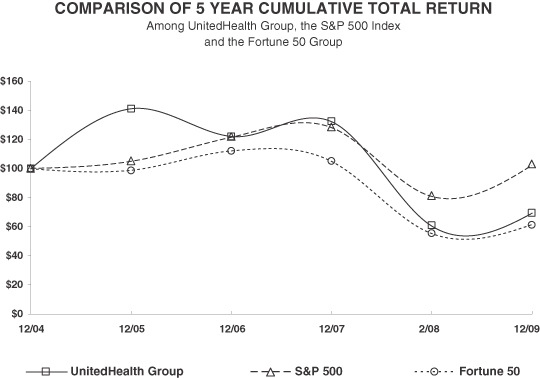
| 12/04 | 12/05 | 12/06 | 12/07 | 12/08 | 12/09 | |||||||||||||
UnitedHealth Group | $ | 100.00 | $ | 141.22 | $ | 122.18 | $ | 132.41 | $ | 60.57 | $ | 69.51 | ||||||
S&P 500 | 100.00 | 104.91 | 121.48 | 128.16 | 80.74 | 102.11 | ||||||||||||
Fortune 50 Group | 100.00 | 99.04 | 112.31 | 105.03 | 55.31 | 61.84 | ||||||||||||
The stock price performance included in this graph is not necessarily indicative of future stock price performance.
28
Peer Group
The companies included in our peer group are Aetna Inc., Cigna Corporation, Coventry Health Care, Inc., Humana Inc. and WellPoint, Inc. We believe that this peer group reflects our peers in the health care industry.
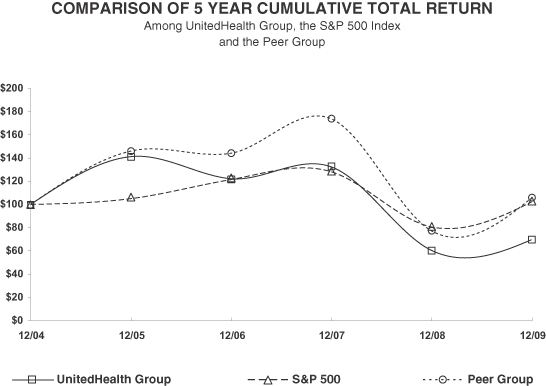
| 12/04 | 12/05 | 12/06 | 12/07 | 12/08 | 12/09 | |||||||||||||
UnitedHealth Group | $ | 100.00 | $ | 141.22 | $ | 122.18 | $ | 132.41 | $ | 60.57 | $ | 69.51 | ||||||
S&P 500 | 100.00 | 104.91 | 121.48 | 128.16 | 80.74 | 102.11 | ||||||||||||
Peer Group | 100.00 | 146.00 | 144.14 | 173.91 | 77.52 | 105.61 | ||||||||||||
The stock price performance included in this graph is not necessarily indicative of future stock price performance.
29
| ITEM 6. | SELECTED FINANCIAL DATA |
FINANCIAL HIGHLIGHTS
| For the Year Ended December 31, | ||||||||||||||||||||
(in millions, except percentages and per share data) | 2009 (a,b) | 2008 (a,b) | 2007 (a,b) | 2006 (a,b) | 2005 (b) | |||||||||||||||
Consolidated Operating Results | ||||||||||||||||||||
Revenues | $ | 87,138 | $ | 81,186 | $ | 75,431 | $ | 71,542 | $ | 46,425 | ||||||||||
Earnings from operations | 6,359 | 5,263 | 7,849 | 6,984 | 5,080 | |||||||||||||||
Net earnings | 3,822 | 2,977 | 4,654 | 4,159 | 3,083 | |||||||||||||||
Return on shareholders' equity | 17.3 | % | 14.9 | % | 22.4 | % | 22.2 | % | 25.2 | % | ||||||||||
Basic net earnings per common share | $ | 3.27 | $ | 2.45 | $ | 3.55 | $ | 3.09 | $ | 2.44 | ||||||||||
Diluted net earnings per common share | 3.24 | 2.40 | 3.42 | 2.97 | 2.31 | |||||||||||||||
Common stock dividends per share | 0.030 | 0.030 | 0.030 | 0.030 | 0.015 | |||||||||||||||
Consolidated Cash Flows From (Used For) | ||||||||||||||||||||
Operating activities | $ | 5,625 | $ | 4,238 | $ | 5,877 | $ | 6,526 | $ | 4,083 | ||||||||||
Investing activities | (976 | ) | (5,072 | ) | (4,147 | ) | (2,101 | ) | (3,489 | ) | ||||||||||
Financing activities | (2,275 | ) | (605 | ) | (3,185 | ) | 474 | 836 | ||||||||||||
Consolidated Financial Condition | ||||||||||||||||||||
(As of December 31) | ||||||||||||||||||||
Cash and investments | $ | 24,350 | $ | 21,575 | $ | 22,286 | $ | 20,582 | $ | 14,982 | ||||||||||
Total assets | 59,045 | 55,815 | 50,899 | 48,320 | 41,288 | |||||||||||||||
Total commercial paper and long-term debt | 11,173 | 12,794 | 11,009 | 7,456 | 7,095 | |||||||||||||||
Shareholders' equity | 23,606 | 20,780 | 20,063 | 20,810 | 17,815 | |||||||||||||||
Debt-to-total-capital ratio | 32.1 | % | 38.1 | % | 35.4 | % | 26.4 | % | 28.5 | % | ||||||||||
Financial Highlights should be read with the accompanying Management's Discussion and Analysis of Financial Condition and Results of Operations and Consolidated Financial Statements and Notes to the Consolidated Financial Statements.
| (a) | On January 1, 2006, we began serving as a plan sponsor offering Medicare Part D drug insurance coverage under a contract with CMS. Total revenues generated under this program were $6.4 billion, $5.8 billion, $5.9 billion and $5.7 billion for the years ended December 31, 2009, 2008, 2007 and 2006, respectively. See Note 2 of Notes to the Consolidated Financial Statements for a detailed discussion of this program. |
| (b) | We acquired Unison Health Plans in May 2008 for total consideration of approximately $930 million, Sierra Health Services, Inc. in February 2008 for total consideration of approximately $2.6 billion, Fiserv Health, Inc. in January 2008 for total consideration of approximately $740 million and PacifiCare Health Systems, Inc. in December 2005 for total consideration of approximately $8.8 billion. The results of operations and financial condition of these acquisitions have been included in our Consolidated Financial Statements since the respective acquisition dates. |
30
| ITEM 7. | MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
The following discussion should be read together with the accompanying Consolidated Financial Statements and Notes to the Consolidated Financial Statements thereto. Readers should be cautioned that the statements, estimates, projections or outlook contained in this report, including discussions regarding financial prospects, economic conditions, trends and uncertainties contained in this Item 7, may constitute forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995, or PSLRA. These forward-looking statements involve risks and uncertainties that may cause our actual results to differ materially from the results discussed in the forward-looking statements. A description of some of the risks and uncertainties can be found in Item 1A, "Risk Factors."
EXECUTIVE OVERVIEW
General
UnitedHealth Group is a diversified health and well-being company, serving more than 70 million Americans. Our focus is on improving the overall health and well-being of the people we serve and their communities and enhancing the performance of the health system. We work with health care professionals and other key partners to expand access to high quality health care. We help people get the care they need at an affordable cost, support the physician/patient relationship, and empower people with the information, guidance and tools they need to make personal health choices and decisions.
Through our diversified family of businesses, we leverage core competencies in advanced technology-based transactional capabilities; health care data, knowledge and information; and health care resource organization and care facilitation to make health care work better. These core competencies are focused in two market areas, health benefits and health services. Health benefits are offered in the individual and employer markets and the public and senior markets through our UnitedHealthcare, Ovations and AmeriChoice businesses. Health services are provided to the participants in the health system itself, ranging from employers and health plans to physicians and life sciences companies through our OptumHealth, Ingenix and Prescription Solutions businesses. In aggregate, these businesses have more than two dozen distinct business units that address specific end markets. Each of these business units focuses on the key goals in health and well-being: access, affordability, quality and simplicity as they apply to their specific market.
Revenues
Our revenues are primarily comprised of premiums derived from risk-based health insurance arrangements in which the premium is fixed, typically for a one-year period, and we assume the economic risk of funding our customers' health care benefits and related administrative costs. We also generate revenues from services performed for customers that self-insure the health care costs of their employees and employees' dependants. For both risk-based and fee-based health care benefit arrangements, we provide coordination and facilitation of medical services; transaction processing; health care professional services; and access to contracted networks of physicians, hospitals and other health care professionals. We also generate service revenues from Ingenix health intelligence and contract research businesses. Product revenues are mainly comprised of products sold by our Prescription Solutions pharmacy benefit management business and sales of Ingenix publishing and software products. We derive investment income primarily from interest earned on our investments in debt securities. Our investment income also includes gains or losses when the securities are sold, or other-than-temporarily impaired.
Operating Costs
Medical Costs. Our operating results depend in large part on our ability to effectively estimate, price for and manage our medical costs through underwriting criteria, product design, negotiation of favorable provider contracts and medical management programs. Controlling medical costs requires a comprehensive and integrated approach to organize and advance the full range of interrelationships among patients/consumers, health professionals, hospitals, pharmaceutical/technology manufacturers and other key stakeholders.
31
Medical costs include estimates of our obligations for medical care services rendered on behalf of insured consumers for which we neither have received nor processed claims, and for liabilities for physician, hospital and other medical cost disputes. In every reporting period, our operating results include the effects of more completely developed medical costs payable estimates associated with previously reported periods.
Our medical care ratio, calculated as medical costs as a percentage of premium revenues, reflects the combination of pricing, benefit designs, consumer health care utilization and comprehensive care facilitation efforts. We seek to sustain a stable medical care ratio for an equivalent mix of business, however, changes in business mix, such as expanding participation in comparatively higher medical care ratio government-sponsored public sector programs, will change the dynamics of our results.
Operating Costs. Operating costs are primarily comprised of costs related to employee compensation and benefits, agent and broker commissions, premium taxes and assessments, professional fees, advertising and occupancy costs.
Cash Flows
We generate cash primarily from premiums, service revenues and investment income, as well as proceeds from the sale or maturity of our investments. Our primary uses of cash are for payments of medical claims, purchases of investments, common stock repurchases and payments on long-term debt. For more information on our cash flows, see "Liquidity" below.
Business Trends
Our businesses participate in the U.S. health economy, which comprises approximately 17% of U.S. gross domestic product and which has grown consistently for many years. We expect overall spending on health care in the U.S. to continue to rise in the future, based on inflation, demographic trends in the U.S. population and national interest in health and well-being. The rate of market growth may be affected by a variety of factors, including macro-economic conditions and proposed health care reforms, which could also impact our results of operations.
Adverse Economic Conditions. The current U.S. recessionary economic environment has impacted demand for some of our products and services. For example, decreases in employment have reduced the number of workers and dependants offered health care benefits by our employer customers, putting pressure on top line growth for our UnitedHealthcare and OptumHealth businesses. This workplace attrition contributed more than half of the 7% decrease in UnitedHealthcare's commercial membership during 2009, and this attrition trend is expected to continue at a generally elevated level until national employment stabilizes. In contrast, our AmeriChoice business is experiencing growth in its state Medicaid offerings as employment rates fall. If the recessionary economic environment continues for a prolonged period, federal and state governments may decrease funding for various health care government programs in which we participate and/or impose new or higher levels of taxes or assessments. Our revenues are also impacted by U.S. monetary and fiscal policy. In response to recessionary conditions, the U.S. Federal Reserve has maintained the target federal funds rate at a range of zero to 25 basis points. Changes in federal monetary policy have reduced the level of investment income received on our portfolio on a year-over-year basis.
In total, we believe that economic recessions will slow our revenue growth rate and could impact our operating profitability. We also believe that government funding pressure, coupled with recessionary economic conditions, will impact the financial positions of hospitals, physicians and other care providers and could therefore increase medical cost trends experienced by our businesses. For additional discussions regarding how the adverse economic conditions could affect our business, see Item 1A, "Risk Factors."
32
American Recovery and Reinvestment Act. Our businesses may benefit from elements of the federal economic stimulus package that was enacted in response to the current recession. These elements include expansion of funding to state programs, which could mitigate funding pressure for AmeriChoice Medicaid offerings at the state level, and funding for health care information technology, which could expand market opportunities for Ingenix.
Proposed Health Care Reforms and Reimbursement Changes. Both houses of Congress have recently passed bills relating to health care reform, which have not yet been reconciled with each other and signed into law. Examples of health care reform proposals include policy changes that would change the dynamics of the health care industry, including having the federal or one or more state governments assume a larger role in the health care system such as competing with private health insurers, imposing new and potentially significant taxes on health insurers and health care benefits, guaranteed coverage requirements, elimination of pre-existing condition exclusions or annual lifetime maximum limits, restrictions on our ability to price products based on our underwriting standards, or restructuring the Medicare or Medicaid programs, including reducing payments over the intermediate term to private plans offering Medicare Advantage. We cannot predict if any of these proposals will ultimately become law, or, if enacted, what their terms or the regulations promulgated pursuant to such laws will be. Any health care reforms enacted may be phased in over a number of years, but, if enacted, could reduce our revenues, increase our costs, expose us to expanded liability and require us to revise the ways in which we conduct business or put us at risk for loss of business. In addition, our operating results, our financial position, including our ability to maintain the value of our goodwill, and cash flows could be materially adversely affected by such changes.
The administration and various congressional leaders have advanced proposals to reduce payments over the intermediate term to private plans offering Medicare Advantage. Further, Centers for Medicare and Medicaid Services (CMS) implemented a reduction in Medicare Advantage reimbursements of approximately 5% for 2010. Although we have adjusted members' benefits and premiums on a selective basis, terminated benefit plans in certain counties, and intensified both our medical and operating cost management in response to these rate reductions, there can be no assurance that we will be able to execute successfully on these or other strategies to address changes in the Medicare Advantage program. Our operating results, financial position and cash flows could be materially adversely affected by these reductions. If industry-wide Medicare Advantage membership declines, there is likely to be increased demand for Medicare Supplemental insurance and Part D prescription drug coverage, and in both categories Ovations is a market leader.
We operate a diversified set of health care focused businesses; this business model has been intentionally designed to address a multitude of market sectors. Therefore, we could see simultaneous increases and decreases in demand for our various products and services, depending on the scope, shape and timing of health care reforms. It is difficult to predict the outcome of reform discussions with precision over the mid- to long-term time horizon. For discussions regarding our risks related to health care reforms, see Item 1A, "Risk Factors."
33
RESULTS SUMMARY
The following summarizes the consolidated financial results for the years ended December 31:
(in millions, except percentages and per | Increase (Decrease) | Increase (Decrease) | ||||||||||||||||||||||||||||||||||
| 2009 | 2008 | 2007 | 2009 vs. 2008 | 2008 vs. 2007 | ||||||||||||||||||||||||||||||||
REVENUES: | ||||||||||||||||||||||||||||||||||||
Premiums | $ | 79,315 | $ | 73,608 | $ | 68,781 | $ | 5,707 | 8 | % | $ | 4,827 | 7 | % | ||||||||||||||||||||||
Services | 5,306 | 5,152 | 4,608 | 154 | 3 | 544 | 12 | |||||||||||||||||||||||||||||
Products | 1,925 | 1,655 | 898 | 270 | 16 | 757 | 84 | |||||||||||||||||||||||||||||
Investment and other income | 592 | 771 | 1,144 | (179 | ) | (23 | ) | (373 | ) | (33 | ) | |||||||||||||||||||||||||
Total revenues | 87,138 | 81,186 | 75,431 | 5,952 | 7 | 5,755 | 8 | |||||||||||||||||||||||||||||
OPERATING COSTS: | ||||||||||||||||||||||||||||||||||||
Medical costs | 65,289 | 60,359 | 55,435 | 4,930 | 8 | 4,924 | 9 | |||||||||||||||||||||||||||||
Medical care ratio | 82.3 | % | 82.0 | % | 80.6 | % | 0.3 | 1.4 | ||||||||||||||||||||||||||||
Operating costs | 12,734 | 13,103 | 10,583 | (369 | ) | (3 | ) | 2,520 | 24 | |||||||||||||||||||||||||||
Operating cost ratio | 14.6 | % | 16.1 | % | 14.0 | % | (1.5 | ) | 2.1 | |||||||||||||||||||||||||||
Cost of products sold | 1,765 | 1,480 | 768 | 285 | 19 | 712 | 93 | |||||||||||||||||||||||||||||
Depreciation and amortization | 991 | 981 | 796 | 10 | 1 | 185 | 23 | |||||||||||||||||||||||||||||
Total operating costs | 80,779 | 75,923 | 67,582 | 4,856 | 6 | 8,341 | 12 | |||||||||||||||||||||||||||||
EARNINGS FROM OPERATIONS | 6,359 | 5,263 | 7,849 | 1,096 | 21 | (2,586 | ) | (33 | ) | |||||||||||||||||||||||||||
Operating margin | 7.3 | % | 6.5 | % | 10.4 | % | 0.8 | (3.9 | ) | |||||||||||||||||||||||||||
Interest expense | (551 | ) | (639 | ) | (544 | ) | (88 | ) | (14 | ) | 95 | 17 | ||||||||||||||||||||||||
EARNINGS BEFORE INCOME TAXES | 5,808 | 4,624 | 7,305 | 1,184 | 26 | (2,681 | ) | (37 | ) | |||||||||||||||||||||||||||
Provision for income taxes | (1,986 | ) | (1,647 | ) | (2,651 | ) | 339 | 21 | (1,004 | ) | (38 | ) | ||||||||||||||||||||||||
Tax rate | 34.2 | % | 35.6 | % | 36.3 | % | (1.4 | ) | (0.7 | ) | ||||||||||||||||||||||||||
NET EARNINGS | $ | 3,822 | $ | 2,977 | $ | 4,654 | $ | 845 | 28 | % | $ | (1,677 | ) | (36 | ) | % | ||||||||||||||||||||
DILUTED NET EARNINGS PER COMMON SHARE | $ | 3.24 | $ | 2.40 | $ | 3.42 | $ | 0.84 | 35 | % | $ | (1.02 | ) | (30 | ) | % | ||||||||||||||||||||
RETURN ON EQUITY | 17.3 | % | 14.9 | % | 22.4 | % | 2.4 | % | (7.5 | ) | % | |||||||||||||||||||||||||
TOTAL PEOPLE SERVED | 70 | 73 | 71 | (3 | ) | (4 | ) | % | 2 | 3 | % | |||||||||||||||||||||||||
ACQUISITIONS
AIM Healthcare Services, Inc. On June 1, 2009, we acquired all of the outstanding shares of AIM Healthcare Services, Inc. (AIM) for approximately $440 million in cash. AIM is a leading provider of payment accuracy solutions for health care payer and hospital clients in all 50 states. This acquisition strengthened our capabilities to simplify and improve administration in the health care industry. The results of operations and financial condition of AIM have been included in our consolidated results and the results of the Ingenix reporting segment since the acquisition date.
Unison Health Plans. On May 30, 2008, we acquired all of the outstanding shares of Unison Health Plans (Unison) for approximately $930 million in cash. Unison provides government-sponsored health plan coverage to people in Pennsylvania, Ohio, Tennessee, Delaware, South Carolina and Washington, D.C. through a network of independent health care professionals. This acquisition strengthened our resources and capabilities in these areas. The results of operations and financial condition of Unison have been included in our consolidated results and the results of our Health Benefits reporting segment since the acquisition date.
34
Sierra Health Services, Inc. On February 25, 2008, we acquired all of the outstanding shares of Sierra Health Services, Inc. (Sierra), a diversified health care services company based in Las Vegas, Nevada, for approximately $2.6 billion in cash, representing a price of $43.50 per share of Sierra common stock. This acquisition strengthened our position in the southwest region of the United States. The U.S. Department of Justice approved the acquisition conditioned upon the divestiture of our individual Medicare Advantage HMO plans in Clark and Nye Counties, Nevada, which represented approximately 30,000 members. The divestiture was completed on April 30, 2008. We received proceeds of $185 million for this transaction, which were recorded as a reduction to Operating Costs. Group Medicare Advantage plans offered through commercial contracts were excluded from the divestiture. Also, we retained Sierra's Medicare Advantage HMO plans in Nevada. The results of operations and financial condition of Sierra have been included in our consolidated results and the results of the Health Benefits, OptumHealth and Prescription Solutions reporting segments since the acquisition date.
Fiserv Health, Inc. On January 10, 2008, we acquired all of the outstanding shares of Fiserv Health, Inc. (Fiserv Health), a subsidiary of Fiserv, Inc., for approximately $740 million in cash. Fiserv Health is a leading administrator of medical benefits and also provides care facilitation services, specialty health solutions and pharmacy benefit management (PBM) services. This transaction allows us to expand the capacity of our existing benefits administration businesses and enables existing and new customers to leverage our full range of assets, including ancillary services, our national network and technology tools. The results of operations and financial condition of Fiserv Health have been included in our consolidated results and the results of the Health Benefits, OptumHealth, Ingenix and Prescription Solutions reporting segments since the acquisition date.
For the years ended December 31, 2009, 2008 and 2007, aggregate consideration paid, net of cash assumed for smaller acquisitions was $95 million, $94 million and $262 million, respectively. These acquisitions were not material to our results of operations.
2009 RESULTS OF OPERATIONS COMPARED TO 2008 RESULTS
Consolidated Financial Results
Revenues
Consolidated revenues for 2009 increased primarily due to the increase in premium revenues in the Health Benefits reporting segment. The increase in premium revenues was primarily due to strong organic growth in risk-based offerings in our public and senior markets businesses and premium rate increases in response to growth in underlying medical costs, partially offset by a decline in the number of people served in the commercial market. The effect of 2008 Health Benefits acquisitions also contributed to the increase in premium revenues during 2009.
Medical Costs
Medical costs for 2009 increased primarily due to growth in public and senior markets risk-based businesses, elevated medical costs due to the H1N1 influenza virus, unemployment-related benefit continuation programs due to an increased level of national unemployment, medical cost inflation and increased utilization of medical services.
For each period, our operating results include the effects of revisions in medical cost estimates related to all prior periods. Changes in medical cost estimates related to prior periods, resulting from more complete claim information identified in the current period, are included in total medical costs reported for the current period. For 2009 and 2008, medical costs included $310 million and $230 million, respectively, of net favorable medical cost development related to prior fiscal years.
Operating Costs
Operating costs for 2009 decreased due to certain expenses incurred in 2008 as discussed below and disciplined operating cost management, which were partially offset by increased costs due to acquired and organic business growth and from an increase in state insurance assessments levied against premiums, a portion of which was in lieu of state income taxes in one of the states in which we operate.
35
Operating costs for 2008 included $882 million for settlement of two class action lawsuits related to our historical stock option practices and related legal costs, $350 million for the settlement of class action litigation related to reimbursement for out-of-network medical services, $50 million related to estimated costs to conclude a legal matter and $46 million for employee severance related to operating cost reduction initiatives and other items, partially offset by a $185 million reduction in operating costs for proceeds from the sale of certain assets and membership in the individual Medicare Advantage business in Nevada in May 2008.
Income Tax Rate
Our income tax rate for 2009 decreased primarily due to the favorable resolution of various historical state income tax matters and the change to a premium tax in lieu of an income tax in one of the states in which we operate, which increased operating costs and decreased income taxes.
Reporting Segments
We have four reporting segments:
| • | Health Benefits, which includes UnitedHealthcare, Ovations and AmeriChoice; |
| • | OptumHealth; |
| • | Ingenix; and |
| • | Prescription Solutions. |
Transactions between reporting segments principally consist of sales of pharmacy benefit products and services to Health Benefits customers by Prescription Solutions, certain product offerings sold to Health Benefits customers by OptumHealth, and consulting and other services sold to Health Benefits by Ingenix. These transactions are recorded at management's estimate of fair value. Intersegment transactions are eliminated in consolidation.
36
The following summarizes the operating results of our reporting segments:
| Increase (Decrease) | Increase (Decrease) | |||||||||||||||||||||||||
(in millions, except percentages) | 2009 | 2008 | 2007 | 2009 vs. 2008 | 2008 vs. 2007 | |||||||||||||||||||||
Revenues | ||||||||||||||||||||||||||
Health Benefits | $ | 81,341 | $ | 75,857 | $ | 71,199 | $ | 5,484 | 7 | % | $ | 4,658 | 7 | % | ||||||||||||
OptumHealth | 5,528 | 5,225 | 4,921 | 303 | 6 | 304 | 6 | |||||||||||||||||||
Ingenix | 1,823 | 1,552 | 1,304 | 271 | 17 | 248 | 19 | |||||||||||||||||||
Prescription Solutions | 14,452 | 12,573 | 13,249 | 1,879 | 15 | (676 | ) | (5 | ) | |||||||||||||||||
Eliminations | (16,006 | ) | (14,021 | ) | (15,242 | ) | (1,985 | ) | nm | 1,221 | nm | |||||||||||||||
Consolidated revenues | $ | 87,138 | $ | 81,186 | $ | 75,431 | $ | 5,952 | 7 | % | $ | 5,755 | 8 | % | ||||||||||||
Earnings from Operations | ||||||||||||||||||||||||||
Health Benefits | $ | 4,788 | $ | 5,068 | $ | 6,595 | $ | (280 | ) | (6 | )% | $ | (1,527 | ) | (23 | )% | ||||||||||
OptumHealth | 636 | 718 | 895 | (82 | ) | (11 | ) | (177 | ) | (20 | ) | |||||||||||||||
Ingenix | 246 | 229 | 266 | 17 | 7 | (37 | ) | (14 | ) | |||||||||||||||||
Prescription Solutions | 689 | 363 | 269 | 326 | 90 | 94 | 35 | |||||||||||||||||||
Corporate | - | (1,115 | ) | (176 | ) | 1,115 | nm | (939 | ) | nm | ||||||||||||||||
Consolidated earnings from operations | $ | 6,359 | $ | 5,263 | $ | 7,849 | $ | 1,096 | 21 | % | $ | (2,586 | ) | (33 | )% | |||||||||||
Operating Margin | ||||||||||||||||||||||||||
Health Benefits | 5.9 | % | 6.7 | % | 9.3 | % | (0.8 | )% | (2.6 | )% | ||||||||||||||||
OptumHealth | 11.5 | 13.7 | 18.2 | (2.2 | ) | (4.5 | ) | |||||||||||||||||||
Ingenix | 13.5 | 14.8 | 20.4 | (1.3 | ) | (5.6 | ) | |||||||||||||||||||
Prescription Solutions | 4.8 | 2.9 | 2.0 | 1.9 | 0.9 | |||||||||||||||||||||
Consolidated operating margin | 7.3 | % | 6.5 | % | 10.4 | % | 0.8 | % | (3.9 | )% | ||||||||||||||||
nm = not meaningful
The following summarizes the number of individuals served by our Health Benefits segment, by major market segment and funding arrangement, at December 31:
| Increase (Decrease) | Increase (Decrease) | |||||||||||||||||
(in thousands, except percentages) | 2009 | 2008 | 2007 | 2009 vs. 2008 | 2008 vs. 2007 | |||||||||||||
Commercial risk-based | 9,415 | 10,360 | 10,805 | (945 | ) | (9 | )% | (445 | ) | (4 | )% | |||||||
Commercial fee-based | 15,210 | 15,985 | 14,720 | (775 | ) | (5 | ) | 1,265 | 9 | |||||||||
Total commercial | 24,625 | 26,345 | 25,525 | (1,720 | ) | (7 | ) | 820 | 3 | |||||||||
Medicare Advantage | 1,790 | 1,495 | 1,370 | 295 | 20 | 125 | 9 | |||||||||||
Medicaid | 2,900 | 2,515 | 1,710 | 385 | 15 | 805 | 47 | |||||||||||
Standardized Medicare supplement | 2,680 | 2,540 | 2,400 | 140 | 6 | 140 | 6 | |||||||||||
Total public and senior | 7,370 | 6,550 | 5,480 | 820 | 13 | 1,070 | 20 | |||||||||||
Total people served by Health Benefits | 31,995 | 32,895 | 31,005 | (900 | ) | (3 | )% | 1,890 | 6 | % | ||||||||
37
Health Benefits
Revenue growth in Health Benefits for 2009 was primarily due to growth in the number of individuals served by our public and senior markets businesses and premium rate increases, partially offset by a decline in individuals served through commercial products and a decrease in investment and other income driven by lower short-term investment yields. UnitedHealthcare revenues of $40.8 billion for 2009 decreased by $1.0 billion, or 2%, compared to 2008, as the reduction in individuals served was partially offset by premium rate increases. Ovations revenues of $32.1 billion for 2009 increased by $4.1 billion, or 15%, over 2008, primarily due to an increase in individuals served through Medicare Part D, Medicare Advantage and standardized Medicare Supplement offerings, as well as premium rate increases. AmeriChoice generated revenues of $8.4 billion for 2009, an increase of $2.4 billion, or 40%, over the comparable 2008 period, primarily due to an increase in the number of individuals served by Medicaid plans and premium rate increases as well as the full year impact from the mid-2008 Unison acquisition.
The decrease in Health Benefits earnings from operations for 2009 was primarily due to a $166 million reduction in investment and other income and a decrease in commercial business, partially offset by the growth in lower margin public and senior markets businesses. The 2009 UnitedHealthcare medical care ratio increased to 84.0% from 83.5% in 2008, largely due to elevated medical costs related to the H1N1 influenza virus and a higher proportion of participants receiving care under unemployment-related benefit continuation programs. Health Benefits' operating margins decreased due to the factors that decreased earnings from operations.
OptumHealth
Increased OptumHealth revenues for 2009 were primarily driven by new business development in large-scale public sector care and behavioral health programs for state clients, which were partially offset by a decline in individuals served through commercial products. As of December 31, 2009 and 2008, OptumHealth provided services to approximately 58 million and 60 million consumers, respectively.
Earnings from operations and operating margins for 2009 decreased due to the decrease in commercial membership described above, start-up costs for new large contracts and lower investment income, partially offset by earnings growth from expanding services in the public sector and disciplined operating cost management.
Ingenix
Improvements in Ingenix revenues and earnings from operations for 2009 were primarily due to the impact of improved performance in the payer business, new internal service offerings and the effect of 2009 acquisitions. The decreases in operating margins for 2009 were primarily due to investments in services offerings, including outsourcing services for pharmaceutical customers and costs for international expansion, hospital revenue cycle management and data privacy and security.
Prescription Solutions
The increased Prescription Solutions revenues for 2009 were primarily due to growth in customers served through Medicare Part D prescription drug plans by our Ovations business, which is the largest customer of this reporting segment. Intersegment revenues eliminated in consolidation were $12.6 billion and $11.0 billion for 2009 and 2008, respectively.
Prescription Solutions earnings from operations for 2009 increased primarily due to prescription volume growth, strong success under performance-based purchasing arrangements, gains in mail service drug fulfillment and a continuing favorable mix shift to generic pharmaceuticals.
38
2008 RESULTS COMPARED TO 2007 RESULTS
Consolidated Financial Results
Revenues
Consolidated revenues for 2008 increased from 2007 primarily due to the increase in premium revenue in the Health Benefits reporting segment. The premium revenue growth generated by our Health Benefits reporting segment was the primary driver in the consolidated premium revenues increase. This increase was due to the growth in individuals served by public and senior markets businesses, premium rate increases for medical cost inflation and acquisitions completed in 2008, partially offset by a decline in individuals served through both UnitedHealthcare risk-based products and Medicare Part D prescription drug plans.
Investment and Other Income. The decrease in investment and other income in 2008 was primarily due to lower investment yields primarily because of the decrease in interest rates on our cash equivalents, decreased average investment balances related to lower operating cash flows, decreased deposits held for certain government-sponsored programs and increased other-than-temporary impairment charges related to the disruption in the financial markets.
Medical Costs
Medical costs for 2008 increased primarily due to medical cost inflation, acquisitions completed in 2008 and growth in Ovations Medicare Advantage and Medicare Supplement products, partially offset by a decrease in the number of individuals served through both UnitedHealthcare risk-based products and Medicare Part D prescription drug plans. For 2008 and 2007, medical costs included $230 million and $420 million, respectively, of net favorable medical cost development related to prior fiscal years.
Operating Costs
The operating cost ratio increased in 2008 primarily due to certain expenses as described in "2009 Results of Operations Compared to 2008 Results" above, acquisitions completed in 2008, costs for anticipated revenue growth that did not fully materialize and a change in business mix towards service revenues from fee-based businesses.
Operating costs for 2007 include $176 million of expenses recorded in the first quarter of 2007 related to application of deferred compensation rules under Section 409A of the Internal Revenue Code (Section 409A) to our historical stock option practices. The $176 million Section 409A charge includes $87 million of expenses for the payment of certain optionholders' tax obligations for stock options exercised in 2006 and early 2007 and $89 million of expenses for the modification related to increasing the exercise price of unexercised stock options granted to nonexecutive officer employees and the related cash payments. For an expanded discussion of our Section 409A charges, see Note 12 of Notes to the Consolidated Financial Statements.
Depreciation and Amortization
The increase in depreciation and amortization was primarily related to higher levels of computer equipment and capitalized software as a result of technology development and enhancements, as well as additional depreciation and amortization related to business acquisitions.
Income Tax Rate
The decrease in our effective income tax rate was primarily due to lower earnings resulting in an increased proportion of tax-free investment income to total earnings.
39
Reporting Segments
Health Benefits
The revenue growth in Health Benefits for 2008 was primarily due to growth in the number of individuals served by our Public and Senior Markets Group, premium rate increases for medical cost inflation and the 2008 acquisitions of Sierra, Fiserv Health, and Unison, partially offset by an organic decline in individuals served through commercial risk-based products and Medicare Part D products and a decrease in investment income. UnitedHealthcare revenues of $41.8 billion in 2008 increased over the comparable 2007 period by $1.6 billion, or 4%. The UnitedHealthcare increase was primarily driven by the same factors as discussed for Health Benefits in 2008. Ovations revenues of $28.1 billion in 2008 increased over the comparable 2007 period by $1.6 billion, or 6%. The increase was primarily due to an increase in individuals served with the standardized Medicare Supplement and Medicare Advantage products gained through both organic growth and the Sierra acquisition and premium rate increases, which were partially offset by a net organic decrease of 675,000 stand-alone Medicare Part D members primarily due to the reassignment by CMS of certain dual-eligible low income beneficiaries based on annual price bids. AmeriChoice generated revenues of $6.0 billion in 2008, an increase of $1.5 billion, or 34%, over the comparable 2007 period, primarily due to an increase in the number of individuals served by Medicaid plans, premium rate increases and the acquisition of Unison in the second quarter of 2008.
The decrease in Health Benefits earnings from operations was primarily due to pressure on enrollment and gross margins in the UnitedHealthcare risk-based business and pressure on gross margins in Medicare Part D prescription drug plans, partially offset by acquisitions. The UnitedHealthcare medical care ratio increased to 83.5% in 2008 from 82.6% in 2007. This increase was primarily driven by the effects of a competitive pricing environment where price increases, net of customer benefit package changes, did not fully match the rise in medical costs, and an increased mix of national account pharmaceutical benefit business, which typically carries a higher medical care ratio. Health Benefits' operating margin was 6.7% for the year ended December 31, 2008, a decrease from 9.3% in 2007 primarily driven by the factors discussed above.
The number of individuals served with commercial products increased due to acquisitions, which included the addition of 1,315,000 fee-based members from Fiserv Health and the addition of 310,000 risk-based individuals gained through the Sierra acquisition. These additions were partially offset by a net decline in individuals served with commercial products of 805,000, or 3%, from December 31, 2007, primarily due to a decline in individuals served with commercial risk-based products and the impact of a competitive commercial risk-based pricing environment. The number of individuals served by Medicare Advantage products at December 31, 2008 increased through the addition of 60,000 seniors from our acquisition of Sierra and organic growth of 95,000 seniors, partially offset by the divestiture of 30,000 individuals in Nevada related to the Sierra acquisition. Medicaid enrollment grew due to the addition of 320,000 and 60,000 individuals from our Unison and Sierra acquisitions, respectively, and strong organic growth of 425,000 individuals.
OptumHealth
Increased revenues in OptumHealth were driven by rate increases for medical cost inflation and an increased number of consumers served by this segment. OptumHealth provided services to approximately 60 million consumers at December 31, 2008, an increase of approximately 1 million individuals year-over-year.
Earnings from operations and operating margin decreased due to the increased costs for risk-based behavioral and specialty benefits businesses and the mix of continued growth in lower margin business.
Ingenix
The improvement in Ingenix revenues was due to continued growth in its health intelligence and contract research businesses as well as from business acquisitions. The decrease in earnings from operations and operating margin was primarily due to excess staffing costs during 2008 for certain research projects, which were cancelled, as well as lower demand for certain consulting services due to the current economic environment.
40
Prescription Solutions
The decreased Prescription Solutions revenues were primarily due to the reduction in the number of individuals served related to the reassignment of dual-eligible beneficiaries described above through Medicare Part D prescription drug plans by our Ovations business, and a shift from name brand pharmaceuticals towards generic utilization, partially offset by revenues related to the Fiserv Health acquisition and growth in business with unaffiliated clients. Intersegment revenues eliminated in consolidation were $11.0 billion and $12.4 billion for 2008 and 2007, respectively.
Prescription Solutions earnings from operations increased primarily due to the Fiserv Health acquisition, gains in mail service drug fulfillment, and a continuing favorable mix shift to generic pharmaceuticals.
LIQUIDITY, FINANCIAL CONDITION AND CAPITAL RESOURCES
Liquidity
Introduction
We manage our liquidity and financial position in the context of our overall business strategy. We continually forecast and manage our cash, investments, working capital balances and capital structure to meet the short- and long-term obligations of our business while maintaining liquidity and financial flexibility. Cash flows generated from operating activities are principally from earnings before depreciation, amortization and other non-cash expenses. As a result, any future decline in our profitability may have a negative impact on our liquidity. The diversity of our businesses, our geographic and customer diversity and our disciplined underwriting and pricing processes for our risk-based businesses, which seek to match premium rate increases with future expected medical costs, partially mitigates the risk of rising medical and operating costs.
Our regulated subsidiaries generate significant cash flows from operations. A majority of the assets held by our regulated subsidiaries are in the form of cash, cash equivalents and investments. After considering expected cash flows from operating activities, we generally invest cash of regulated subsidiaries that exceeds our expected short-term obligations in longer term, investment-grade, marketable debt securities to improve our overall investment return. We make these investments pursuant to our Board of Directors' approved investment policy, which focuses on preservation of capital, credit quality, diversification, income and duration. The policy also generally governs return objectives, regulatory limitations, tax implications and risk tolerances.
Our regulated subsidiaries are subject to regulations and standards in their respective states of domicile. Most of these regulations and standards conform to those established by the National Association of Insurance Commissioners. These standards, among other things, require these subsidiaries to maintain specified levels of statutory capital, as defined by each state, and restrict the timing and amount of dividends and other distributions that may be paid to their parent companies. Except in the case of extraordinary dividends, these standards generally permit dividends to be paid from statutory unassigned surplus of the regulated subsidiary and are limited based on the regulated subsidiary's level of statutory net income and statutory capital and surplus. These dividends are referred to as "ordinary dividends" and generally can be paid without prior regulatory approval. If the dividend, together with other dividends paid within the preceding twelve months, exceeds a specified statutory limit or is paid from sources other than earned surplus, it is generally considered an "extraordinary dividend" and must receive prior regulatory approval.
In 2009, based on the 2008 statutory net income and statutory capital and surplus levels, the maximum amount of ordinary dividends that could be paid was $3.1 billion. For the year ended December 31, 2009, our regulated subsidiaries paid their parent companies dividends of $4.2 billion, including $2.5 billion of extraordinary dividends. For the year ended December 31, 2008, our regulated subsidiaries paid their parent companies dividends of $4.2 billion, including $1.2 billion of extraordinary dividends. The increase in the proportion of extraordinary dividends to total dividends in 2009 primarily reflects the acceleration of dividend timing, as well as the size of specific dividends beyond ordinary levels. Given expected statutory capital levels, we anticipate lower overall regulated subsidiary dividends in 2010.
41
Our non-regulated businesses also generate cash flows from operations for general corporate use. Cash flows generated by these entities, combined with dividends from our regulated entities and financing through the issuance of commercial paper and long-term debt, as well as the availability of our committed credit facility, further strengthen our operating and financial flexibility. We generally use these cash flows to reinvest in our businesses through capital expenditures, expanding our services through business acquisitions, repaying debt and/or repurchasing shares of our common stock, depending on market conditions.
Results
A summary of our major sources and uses of cash is reflected in the table below:
| Year Ended December 31, | ||||||||||||
(in millions) | 2009 | 2008 | 2007 | |||||||||
Sources of Cash: | ||||||||||||
Cash provided by operating activities | $ | 5,625 | $ | 4,238 | $ | 5,877 | ||||||
Sales of investments | 4,040 | 5,568 | 1,271 | |||||||||
Maturities of investments | 2,675 | 3,030 | 2,094 | |||||||||
Issuance of long-term debt | - | 2,981 | 3,582 | |||||||||
Interest rate swap termination | 513 | - | - | |||||||||
Other | 546 | 1,770 | 1,962 | |||||||||
Total sources of cash | 13,399 | 17,587 | 14,786 | |||||||||
Uses of Cash: | ||||||||||||
Purchases of investments | (6,466 | ) | (9,251 | ) | (6,379 | ) | ||||||
Cash paid for acquisitions, net of cash assumed and disposition | (486 | ) | (3,813 | ) | (262 | ) | ||||||
Retirement of long-term debt | (1,350 | ) | (500 | ) | (950 | ) | ||||||
Common stock repurchases | (1,801 | ) | (2,684 | ) | (6,599 | ) | ||||||
Repayments of commercial paper, net | (99 | ) | (1,346 | ) | - | |||||||
Other | (823 | ) | (1,432 | ) | (2,051 | ) | ||||||
Total uses of cash | (11,025 | ) | (19,026 | ) | (16,241 | ) | ||||||
Net increase (decrease) in cash | $ | 2,374 | $ | (1,439 | ) | $ | (1,455 | ) | ||||
2009 Cash Flows Compared To 2008 Cash Flows
Cash flows from operating activities increased $1.4 billion, or 33%, primarily due to the payment in 2008 of $573 million, net of taxes, for the settlement of two class action lawsuits related to our historical stock option practices, the 2009 increase in medical costs payable driven by membership growth in risk-based products in the public and senior markets businesses, and the effect of changes to our receivable and payable balances with CMS related to Medicare Part D. Additionally, we paid less taxes in 2009 due to tax law changes that took effect in 2008. Operating cash flows in 2008 included payment of 2007 taxes due under the prior tax law, while the 2009 payment did not include prior year amounts. We anticipate lower cash flows from operations in 2010 as compared to 2009 as a result of an anticipated decrease in net earnings, the timing of certain CMS payments and the impact of a legislated change to the timing of payments for Medicare Part D claims.
Cash flows used for investing activities decreased $4.1 billion, or 81%, primarily due to acquisitions completed in 2008 and decreases in the usage of cash in 2009 for purchases of investments, which more than offset the 2009 decreases in sales and maturities of investments.
Cash flows used for financing activities increased $1.7 billion due to the issuance of long-term debt in 2008 and the effect of our change in intent with respect to offsetting cash balances in excess of bank deposits in 2008. See Note 2 of Notes to the Consolidated Financial Statements for further detail of our policy on offsetting cash balances. These items were partially offset by decreases in common stock repurchases in 2009 and the 2009 proceeds from our terminated interest rate swap contracts.
42
2008 Cash Flows Compared To 2007 Cash Flows
Cash flows from operating activities decreased $1.6 billion, or 28%, primarily due to the decrease in net earnings, which included payments for the settlement of two class action lawsuits described above.
Cash flows used for investing activities increased $925 million, or 22%, primarily due to acquisitions completed in 2008 and increases in the usage of cash in 2008 for purchases of investments offset by the 2008 decreases in sales and maturities of investments.
Cash flows used for financing activities decreased $2.6 billion, or 81%, primarily due to decreases in common stock repurchases in 2008 offset by the effect of our change in intent with respect to offsetting cash balances in excess of bank deposits in 2008.
Financial Condition
As of December 31, 2009, our cash, cash equivalent and available-for-sale investment balances of $24.2 billion included $9.8 billion of cash and cash equivalents (which included $2.3 billion held by non-regulated entities), $13.8 billion of debt securities and $577 million of equity securities and venture capital funds. Given the significant portion of our portfolio held in cash equivalents, we do not anticipate fluctuations in the aggregate fair value of our financial assets to have a material impact on our liquidity. The use of different market assumptions or valuation methodologies, primarily used in valuing our Level 3 equity securities, may have an effect on the estimated fair value amounts of our investments. Due to the subjective nature of these assumptions, the estimates may not be indicative of the actual exit price if we had sold the investment at the measurement date. Other sources of liquidity, primarily from operating cash flows, reduce the need to sell investments in adverse markets. See Note 5 of Notes to the Consolidated Financial Statements for further detail of our fair value measurements.
Our investment portfolio has a weighted average duration of 2.1 years and a weighted average credit rating of "AA" as of December 31, 2009. Included in the debt securities balance were $3.0 billion of state and municipal obligations that are guaranteed by third parties. A number of different guarantors guarantee the securities, and we do not have any significant exposure to any single guarantor (neither indirect through the guarantees, nor direct through investment in the guarantor). Further, due to the high underlying credit rating of the issuers, the weighted average credit rating of these securities both with and without the guarantee is "AA" as of December 31, 2009.
Capital Resources and Uses of Liquidity
In addition to cash flow from operations and significant cash and cash equivalent balances at our regulated and unregulated entities, our capital resources and uses of liquidity are as follows:
Commercial Paper. We maintain a commercial paper program, which facilitates the issuance of senior unsecured debt sold on a discount basis with maturities of up to 270 days through third-party broker-dealers. The commercial paper program is supported by the $2.5 billion bank credit facility described below. We did not have any commercial paper outstanding as of December 31, 2009.
Bank Credit Facility . We have a five-year revolving bank credit facility with 23 banks, which matures in May 2012. This facility supports our commercial paper program and is available for general corporate purposes. We had no amounts outstanding under this facility as of December 31, 2009. The interest rate is variable based on term and amount and is calculated based on the London Interbank Offered Rate (LIBOR) plus a spread. As of December 31, 2009, the interest rate on this facility, had it been drawn, would have ranged from 0.4% to 0.7%.
Our bank credit facility contains various covenants, the most restrictive of which requires us to maintain a debt-to-total-capital ratio below 50%. Our debt-to-total-capital ratio, calculated as the sum of commercial paper and debt divided by the sum of commercial paper, debt and shareholders' equity, was 32.1% and 38.1% as of December 31, 2009 and December 31, 2008, respectively. We complied with the requirements of all debt covenants as of December 31, 2009.
43
Shelf Registration. In February 2008, we filed a universal S-3 shelf registration statement with the SEC registering an unspecified amount of debt securities.
Credit Ratings. Our credit ratings at December 31, 2009 were as follows:
| Moody's | Standard & Poor's | Fitch | ||||||||||
| Ratings | Outlook | Ratings | Outlook | Ratings | Outlook | |||||||
Senior unsecured debt | Baa1 | Stable | A- | Negative | A- | Negative | ||||||
Commercial paper | P-2 | n/a | A-2 | n/a | F1 | n/a | ||||||
The availability of financing in the form of debt or equity is influenced by many factors, including our profitability, operating cash flows, debt levels, credit ratings, debt covenants and other contractual restrictions, regulatory requirements and economic and market conditions. For example, a significant downgrade in our credit ratings or conditions in the capital markets may increase the cost of borrowing for us or limit our access to capital. We have therefore adopted strategies and actions toward maintaining financial flexibility to mitigate the impact of such factors on our ability to raise capital.
Debt Tender. In February 2010, we completed cash tender offers for $775 million aggregate principal amount of certain of our outstanding notes. We believe this debt repurchase will improve the matching of floating rate assets and liabilities on our balance sheet and reduce our debt service cost. We used cash on hand to fund the purchase of the notes.
Share Repurchases. Under our Board of Directors' authorization, we maintain a common share repurchase program. Repurchases may be made from time to time at prevailing prices in the open market. In 2009, we repurchased 74.3 million shares at an average price of approximately $24 per share and an aggregate cost of $1.8 billion. As of December 31, 2009, we had Board of Directors' authorization to purchase up to an additional 28.7 million shares of our common stock. In February 2010, the Board renewed and increased our share repurchase program, and authorized us to repurchase up to 120 million shares of our common stock.
CONTRACTUAL OBLIGATIONS AND COMMITMENTS
The following table summarizes future obligations due by period as of December 31, 2009, under our various contractual obligations and commitments:
(in millions) | 2010 | 2011 to 2012 | 2013 to 2014 | Thereafter | Total | ||||||||||
Debt (a) | $ | 2,164 | $ | 1,361 | $ | 1,559 | $ | 6,089 | $ | 11,173 | |||||
Interest on debt (b) | 545 | 659 | 406 | 3,549 | 5,159 | ||||||||||
Operating leases | 255 | 420 | 272 | 644 | 1,591 | ||||||||||
Purchase obligations (c) | 115 | 31 | - | - | 146 | ||||||||||
Future policy benefits (d) | 139 | 353 | 337 | 1,152 | 1,981 | ||||||||||
Unrecognized tax benefits (e) | 19 | - | - | 104 | 123 | ||||||||||
Unfunded investment commitments (f) | 138 | 42 | 24 | 16 | 220 | ||||||||||
Other obligations (g) | 210 | 80 | - | 252 | 542 | ||||||||||
Total contractual obligations | $ | 3,585 | $ | 2,946 | $ | 2,598 | $ | 11,806 | $ | 20,935 | |||||
| (a) | See Note 9 of Notes to the Consolidated Financial Statements for more detail. |
| (b) | Calculated using stated rates from the debt agreements and assuming amounts are outstanding through their contractual term, including the effect of the debt tender described in Note 9 of Notes to the Consolidated Financial Statements. For variable-rate obligations, we used the rates in place as of December 31, 2009 to estimate all remaining contractual payments. Includes unamortized discounts from par values. |
| (c) | Includes fixed or minimum commitments under existing purchase obligations for goods and services, including agreements that are cancelable with the payment of an early termination penalty. Excludes agreements that are cancelable without penalty and excludes liabilities to the extent recorded in our Consolidated Balance Sheets as of December 31, 2009. |
44
| (d) | Estimated payments required under life and annuity contracts held by a divested entity. Under our reinsurance arrangement with OneAmerica Financial Partners, Inc. (OneAmerica) these amounts are payable by OneAmerica, but we remain liable to the policyholders if they are unable to pay. We have recorded a corresponding reinsurance receivable from OneAmerica in our Consolidated Financial Statements. |
| (e) | Since the timing of future settlements is uncertain, the long-term portion has been classified as "Thereafter." See Note 10 of Notes to the Consolidated Financial Statements for more detail. |
| (f) | Includes remaining capital commitments for venture capital funds and the investment commitment related to the PacifiCare acquisition. |
| (g) | Includes obligations associated with contingent consideration related to a business acquisition, certain employee benefit programs, and charitable contributions related to the PacifiCare acquisition. Due to uncertainty regarding payment timing, obligations for employee benefit programs and the charitable contributions have been classified as "Thereafter". |
We do not have other significant contractual obligations or commitments that require cash resources; however, we continually evaluate opportunities to expand our operations. This includes internal development of new products, programs and technology applications, and may include acquisitions.
OFF-BALANCE SHEET ARRANGEMENTS
We do not participate or knowingly seek to participate in transactions that generate relationships with unconsolidated entities or financial partnerships, such as entities often referred to as structured finance or special purpose entities (SPEs), which would have been established for the purpose of facilitating off-balance sheet arrangements or other contractually narrow or limited purposes. As of December 31, 2009, we were not involved in any SPE transactions.
RECENTLY ISSUED ACCOUNTING STANDARDS
In October 2009, the Financial Accounting Standards Board (FASB) issued Accounting Standards Update (ASU) No. 2009-13, "Multiple-Deliverable Revenue Arrangements" (ASU 2009-13). This update removes the criterion that entities must use objective and reliable evidence of fair value in separately accounting for deliverables and provides entities with a hierarchy of evidence that must be considered when allocating arrangement consideration. The new guidance also requires entities to allocate arrangement consideration to the separate units of accounting based on the deliverables' relative selling price. The provisions will be effective for revenue arrangements entered into or materially modified in our fiscal year 2011 and must be applied prospectively. We are currently evaluating the impact of the provisions of ASU 2009-13.
We have determined that all other recently issued accounting standards will not have a material impact on our Consolidated Financial Statements, or do not apply to our operations.
CRITICAL ACCOUNTING ESTIMATES
Critical accounting estimates are those estimates that require management to make challenging, subjective or complex judgments, often because they must estimate the effects of matters that are inherently uncertain and may change in subsequent periods. Critical accounting estimates involve judgments and uncertainties that are sufficiently sensitive and may result in materially different results under different assumptions and conditions.
Medical Costs
Each reporting period, we estimate our obligations for medical care services that have been rendered on behalf of insured consumers but for which claims have either not yet been received or processed and for liabilities for physician, hospital and other medical cost disputes. We develop estimates for medical care services incurred but
45
not reported using an actuarial process that is consistently applied, centrally controlled and automated. The actuarial models consider factors such as time from date of service to claim receipt, claim backlogs, seasonal variances in medical care consumption, health care professional contract rate changes, medical care utilization and other medical cost trends, membership volume and demographics, benefit plan changes, and business mix changes related to products, customers and geography. Depending on the health care professional and type of service, the typical billing lag for services can be up to 90 days from the date of service. Substantially all claims related to medical care services are known and settled within nine to twelve months from the date of service. We estimate liabilities for physician, hospital and other medical cost disputes based upon an analysis of potential outcomes, assuming a combination of litigation and settlement strategies.
Each period, we re-examine previously established medical costs payable estimates based on actual claim submissions and other changes in facts and circumstances. As more complete claim information becomes available, we adjust the amount of the estimates and include the changes in estimates in medical costs in the period in which the change is identified. In every reporting period, our operating results include the effects of more completely developed medical costs payable estimates associated with previously reported periods. If the revised estimate of prior period medical costs is less than the previous estimate, we will decrease reported medical costs in the current period (favorable development). If the revised estimate of prior period medical costs is more than the previous estimate, we will increase reported medical costs in the current period (unfavorable development). Medical costs in 2009, 2008 and 2007, included net favorable medical cost development related to prior periods of $310 million, $230 million and $420 million, respectively.
In developing our medical costs payable estimates, we apply different estimation methods depending on the month for which incurred claims are being estimated. For example, we actuarially calculate completion factors using an analysis of claim adjudication patterns over the most recent 36-month period. A completion factor is an actuarial estimate, based upon historical experience, of the percentage of incurred claims during a given period that have been adjudicated by us at the date of estimation. For months prior to the most recent three months, we apply the completion factors to actual claims adjudicated-to-date to estimate the expected amount of ultimate incurred claims for those months. For the most recent three months, we estimate claim costs incurred primarily by applying observed medical cost trend factors to the average per member per month (PMPM) medical costs incurred in prior months for which more complete claim data is available, supplemented by a review of near-term completion factors. Medical cost trend factors are developed through a comprehensive analysis of claims incurred in prior months and by reviewing a broad set of health care utilization indicators including, but not limited to, pharmacy utilization trends, inpatient hospital census data and incidence data from the National Centers for Disease Control. This approach is consistently applied from period to period.
Completion factors are the most significant factors we use in developing our medical costs payable estimates for older periods, generally periods prior to the most recent three months. The following table illustrates the sensitivity of these factors and the estimated potential impact on our medical costs payable estimates for those periods as of December 31, 2009:
Completion Factors Increase (Decrease) in Factors | Increase (Decrease) in Medical Costs Payable | |||
| (in millions) | ||||
(0.75)% | $ | 171 | ||
(0.50) | 114 | |||
(0.25) | 57 | |||
0.25 | (57 | ) | ||
0.50 | (113 | ) | ||
0.75 | (169 | ) | ||
46
Medical cost PMPM trend factors are the most significant factors we use in developing our medical costs payable estimates for the most recent three months. The following table illustrates the sensitivity of these factors and the estimated potential impact on our medical costs payable estimates for the most recent three months as of December 31, 2009:
Medical Cost PMPM Trend | Increase (Decrease) in Medical Costs Payable | |||
| (in millions) | ||||
3% | $ | 332 | ||
2 | 222 | |||
1 | 111 | |||
(1) | (111 | ) | ||
(2) | (222 | ) | ||
(3) | (332 | ) | ||
The analyses above include outcomes that are considered reasonably likely based on our historical experience estimating liabilities for incurred but not reported benefit claims.
Our estimate of medical costs payable represents management's best estimate of our liability for unpaid medical costs as of December 31, 2009, developed using consistently applied actuarial methods. Management believes the amount of medical costs payable is reasonable and adequate to cover our liability for unpaid claims as of December 31, 2009; however, actual claim payments may differ from established estimates. Assuming a hypothetical 1% difference between our December 31, 2009 estimates of medical costs payable and actual medical costs payable, excluding AARP Medicare Supplement Insurance, 2009 net earnings would increase or decrease by $52 million and diluted net earnings per common share would increase or decrease by $0.04 per share.
The current national health care cost inflation rate significantly exceeds the general inflation rate. We use various strategies to lessen the effects of health care cost inflation. These include coordinating care with physicians and other health care professionals and rate discounts from physicians and other health care professionals. Through contracts with physicians and other health care professionals, we emphasize preventive health care, appropriate use of health care services consistent with clinical performance standards, education and closing gaps in care.
We believe our strategies to mitigate the impact of health care cost inflation on our operating results have been and will continue to be successful. However, other factors including competitive pressures, new health care and pharmaceutical product introductions, demands from physicians and other health care professionals and consumers, major epidemics, and applicable regulations may affect our ability to control the impact of health care cost inflation. Because of the narrow operating margins of our risk-based products, changes in medical cost trends that were not anticipated in establishing premium rates can create significant changes in our financial results.
Revenues
Revenues are principally derived from health care insurance premiums. We recognize premium revenues in the period eligible individuals are entitled to receive health care services. Customers are typically billed monthly at a contracted rate per eligible person multiplied by the total number of people eligible to receive services, as recorded in our records. Employer groups generally provide us with changes to their eligible population one month in arrears. Each billing includes an adjustment for prior period changes in eligibility status that were not reflected in our previous billing. We estimate and adjust the current period's revenues and accounts receivable accordingly. Our estimates are based on historical trends, premiums billed, the level of contract renewal activity and other relevant information. We revise estimates of revenue adjustments each period and record changes in the period they become known.
47
CMS deploys a risk adjustment model, which apportions premiums paid to all health plans according to health severity and certain demographic factors. The CMS risk adjustment model pays more for members whose medical history indicates they have certain medical conditions. Under this risk adjustment methodology, CMS calculates the risk adjusted premium payment using diagnosis data from hospital inpatient, hospital outpatient and physician treatment settings. We and other health care providers collect, capture, and submit the necessary and available diagnosis data to CMS within prescribed deadlines. We estimate risk adjustment revenues based upon the diagnosis data submitted and expected to be submitted to CMS.
Goodwill and Intangible Assets
Goodwill. Goodwill represents the amount of the purchase price in excess of the fair values assigned to the underlying identifiable net assets of acquired businesses. Goodwill is not amortized, but is subject to an annual impairment test. Tests are performed more frequently if events occur or circumstances change that would more likely than not reduce the fair value of the reporting unit below its carrying amount. To determine whether goodwill is impaired, we perform a two-step impairment test. In the first step of the test, the fair values of the reporting units are compared to their aggregate carrying values, including goodwill. If the fair value of the reporting unit is greater than its carrying amount, goodwill is not impaired and no further testing is required. If the fair value of the reporting unit is less than its carrying amount, we would proceed to step two of the test. In step two of the test, the implied fair value of the goodwill of the reporting unit is determined by a hypothetical allocation of the fair value calculated in step one to all of the assets and liabilities of that reporting unit (including any recognized and unrecognized intangible assets) as if the reporting unit had been acquired in a business combination and the fair value was reflective of the price paid to acquire the reporting unit. The implied fair value of goodwill is the excess, if any, of the calculated fair value after hypothetical allocation to the reporting unit's assets and liabilities. If the implied fair value of the goodwill is greater than the carrying amount of the goodwill at the analysis date, goodwill is not impaired and the analysis is complete. If the implied fair value of the goodwill is less than the carrying value of goodwill at the analysis date, goodwill is deemed impaired by the amount of that variance.
We calculate the estimated fair value of our reporting units using discounted cash flows. To determine fair values we must make assumptions about a wide variety of internal and external factors. Significant assumptions used in the impairment analysis include financial projections of free cash flow (including significant assumptions about operations, capital requirements and income taxes), long-term growth rates for determining terminal value, and discount rates. Where available and appropriate, comparative market multiples are used to corroborate the results of our discounted cash flow test.
We completed our annual assessment of goodwill as of January 1, 2010 and determined that no impairment existed as of December 31, 2009. Although we believe that the financial projections used are reasonable and appropriate for all of our reporting units, there is uncertainty inherent in those projections. That uncertainty is increased by potential health care reforms as discussed in "Proposed Health Care Reforms and Reimbursement Changes" above, as any passed legislation may significantly change the forecasts and long-term growth rate assumptions for some or all of our reporting units.
Intangible assets. Finite lived intangible assets are acquired in a business combination and are assets that represent future expected benefits but lack physical substance (e.g., customer lists and trademarks). We do not have material holdings of indefinite lived intangible assets. Intangible assets are amortized over their expected useful lives and are subject to impairment tests when events or circumstances indicate that a finite lived intangible asset's (or asset group's) carrying value may exceed its estimated fair value. If the carrying value exceeds its estimated fair value, an impairment would be recorded.
We calculate the estimated fair value of finite lived intangible assets using undiscounted cash flows that are expected to result from the use of the intangible asset or group of assets. We consider many factors, including estimated future utility to estimate cash flows. There were no material impairments of finite lived intangible assets during the current year.
48
Investments
As of December 31, 2009, we had investments with a carrying value of $14.6 billion, primarily held in marketable debt securities. Our investments are principally classified as available-for-sale and are recorded at fair value. We exclude gross unrealized gains and losses on available-for-sale investments from earnings and report net unrealized gains or losses, net of income tax effects, as a separate component in shareholders' equity. We continually monitor the difference between the cost and fair value of our investments. As of December 31, 2009, our investments had gross unrealized gains of $493 million and gross unrealized losses of $50 million. We evaluate investments for impairment considering the length of time and extent to which market value has been less than cost, the financial condition and near-term prospects of the issuer as well as specific events or circumstances that may influence the operations of the issuer and our intent to sell the security or the likelihood that we will be required to sell the security before recovery of the entire amortized cost. For debt securities, if we intend to either sell or determine that we will be more likely than not be required to sell a debt security before recovery of the entire amortized cost basis or maturity of the debt security, we recognize the entire impairment in earnings. If we do not intend to sell the debt security and we determine that we will not be more likely than not be required to sell the debt security but we do not expect to recover the entire amortized cost basis, the impairment is bifurcated into the amount attributed to the credit loss, which is recognized in earnings, and all other causes, which are recognized in other comprehensive income. For equity securities, we recognize impairments in other comprehensive income if we expect to hold the equity security until fair value increases to at least the equity security's cost basis and we expect that increase in fair value to occur in a reasonably forecasted period. If we intend to sell the equity security or if we believe that recovery of fair value to cost will not occur in the near term, we recognize the impairment in net earnings. New information and the passage of time can change these judgments. We manage our investment portfolio to limit our exposure to any one issuer or market sector, and largely limit our investments to U.S. government and agency securities; state and municipal securities; mortgage-backed securities; and corporate debt obligations, substantially all of investment grade quality. Securities downgraded below policy minimums after purchase will be disposed of in accordance with the investment policy.
Income Taxes
Our provision for income taxes, deferred tax assets and liabilities, and uncertain tax positions reflect our assessment of estimated future taxes to be paid on items in the consolidated financial statements. Deferred income taxes arise from temporary differences between financial reporting and tax reporting bases of assets and liabilities, as well as net operating loss and tax credit carryforwards for tax purposes.
We have established a net valuation allowance against certain deferred tax assets for which the ultimate realization of future benefits is uncertain. After application of the valuation allowances, we anticipate that no limitations will apply with respect to utilization of any of the other net deferred income tax assets. We believe that our estimates for the valuation allowances against deferred tax assets and tax contingency reserves are appropriate based on current facts and circumstances.
According to U.S. Generally Accepted Accounting Principles (GAAP), a tax benefit from an uncertain tax position may be recognized when it is more likely than not that the position will be sustained upon examination, including resolutions of any related appeals or litigation processes, based on the technical merits.
We have established an estimated liability for federal, state and non-U.S. income tax exposures that arise and meet the criteria for accrual under U.S. GAAP. We prepare and file tax returns based on our interpretation of tax laws and regulations and record estimates based on these judgments and interpretations. In the normal course of business, our tax returns are subject to examination by various taxing authorities. Such examinations may result in future tax and interest assessments by these taxing authorities. Inherent uncertainties exist in estimates of tax contingencies due to changes in tax law resulting from legislation, regulation and/or as concluded through the various jurisdictions' tax court systems.
49
The significant assumptions and estimates described above are important contributors to our ultimate effective tax rate in each year. A hypothetical increase or decrease in our effective tax rate by 1% on our 2009 earnings before income taxes would have caused the provision for income taxes to change by $58 million.
Contingent Liabilities
Because of the nature of our businesses, we are routinely involved in various disputes, legal proceedings and governmental audits and investigations. We record liabilities for our estimates of the probable costs resulting from these matters. Our estimates are developed in consultation with outside legal counsel, if appropriate, and are based upon an analysis of potential results, assuming a combination of litigation and settlement strategies and considering our insurance coverage, if any, for such matters. It is possible that future results of operations for any particular quarterly or annual period could be materially affected by changes in our estimates or assumptions.
LEGAL MATTERS
A description of our legal proceedings is included in Note 14 of Notes to the Consolidated Financial Statements and is incorporated by reference herein.
CONCENTRATIONS OF CREDIT RISK
Investments in financial instruments such as marketable securities and accounts receivable may subject us to concentrations of credit risk. Our investments in marketable securities are managed under an investment policy authorized by our Board of Directors. This policy limits the amounts that may be invested in any one issuer and generally limits our investments to U.S. government and agency securities, state and municipal securities and corporate debt obligations that are investment grade. Concentrations of credit risk with respect to accounts receivable are limited due to the large number of employer groups that constitute our customer base. As of December 31, 2009, we had an aggregate $2.0 billion reinsurance receivable resulting from the sale of our Golden Rule Financial Corporation life and annuity business in 2005. We regularly evaluate the financial condition of the reinsurer and only record the reinsurance receivable to the extent that the amounts are deemed probable of recovery. Currently, the reinsurer is rated by A.M. Best as "A." As of December 31, 2009, there were no other significant concentrations of credit risk.
| ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
Our primary market risks are exposures to (a) changes in interest rates that impact our investment income and interest expense and the fair value of certain of our fixed-rate financial investments and debt and (b) changes in equity prices that impact the value of our equity investments.
As of December 31, 2009, $9.8 billion of our financial investments were classified as cash and cash equivalents on which interest rates received vary with market interest rates, which may materially impact our investment income. Also, $750 million of our debt as of December 31, 2009 was at interest rates that vary with market rates.
The fair value of certain of our fixed-rate financial investments and debt also varies with market interest rates. As of December 31, 2009, $14.0 billion of our investments were fixed-rate debt securities and $10.4 billion of our debt was fixed-rate term debt. An increase in market interest rates decreases the market value of fixed-rate investments and fixed-rate debt. Conversely, a decrease in market interest rates increases the market value of fixed-rate investments and fixed-rate debt.
We manage exposure to market interest rates by diversifying investments across different fixed income market sectors and debt across maturities and interest rate indices, as well as endeavoring to match our floating rate assets and liabilities over time in normal markets, either directly or through the use of interest rate swap
50
contracts. As part of our risk management strategy, we may enter into interest rate swap agreements with financial institutions to manage the impact of market interest rates on interest expense. In January 2009, we terminated interest rate swap contracts with $4.9 billion in notional value to lock-in the benefit of low market interest rates. This gain will be realized over the remaining life of the applicable hedged fixed-rate debt as a reduction to interest expense in the Consolidated Statements of Operations.
The following table summarizes the impact of a hypothetical change in market interest rates by 1% or 2% as of December 31, 2009 on our investment income and interest expense per annum, and the fair value of our financial investments and debt (in millions):
Increase (Decrease) in Market Interest Rate | Investment Income Per Annum (a) | Interest Expense Per Annum (a) | Fair Value of Financial Investments | Fair Value of Debt | ||||||||||||
2% | $ | 196 | $ | 15 | $ | (1,059 | ) | $ | (1,187 | ) | ||||||
1 | 98 | 8 | (540 | ) | (633 | ) | ||||||||||
(1) | (15 | ) | (6 | ) | 541 | 730 | ||||||||||
(2) | nm | nm | 1,075 | 1,579 | ||||||||||||
nm = not meaningful
| (a) | Given the low absolute level of short-term market rates on our floating rate assets and liabilities as of December 31, 2009, the assumed hypothetical change in interest rates has been floored at zero and does not reflect the full 1% point reduction in interest income or interest expense. |
As of December 31, 2009, we had $577 million of equity securities and venture capital funds, a portion of which were invested in various public and non-public companies concentrated in the areas of health care delivery and related information technologies. Market conditions that affect the value of health care or technology stocks will likewise impact the value of our equity investments.
51
| ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Shareholders of UnitedHealth Group Incorporated and subsidiaries:
We have audited the accompanying consolidated balance sheets of UnitedHealth Group Incorporated and subsidiaries (the "Company") as of December 31, 2009 and 2008, and the related consolidated statements of operations, stockholders' equity and cash flows for each of the three years in the period ended December 31, 2009. These consolidated financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the consolidated financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, such consolidated financial statements present fairly, in all material respects, the financial position of UnitedHealth Group Incorporated and Subsidiaries as of December 31, 2009 and 2008, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2009, in conformity with accounting principles generally accepted in the United States of America.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the Company's internal control over financial reporting as of December 31, 2009, based on the criteria established in Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated February 10, 2010 expressed an unqualified opinion on the Company's internal control over financial reporting.
| / S / DELOITTE & TOUCHE LLP |
| Minneapolis, MN |
| February 10, 2010 |
52
UnitedHealth Group
Consolidated Balance Sheets
| December 31, | ||||||||
(in millions, except per share data) | 2009 | 2008 | ||||||
ASSETS | ||||||||
Current assets: | ||||||||
Cash and cash equivalents | $ | 9,800 | $ | 7,426 | ||||
Short-term investments | 1,239 | 783 | ||||||
Accounts receivable, net of allowances of $220 and $148 | 1,954 | 1,929 | ||||||
Assets under management | 2,383 | 2,199 | ||||||
Deferred income taxes | 448 | 424 | ||||||
Other current receivables | 1,838 | 1,715 | ||||||
Prepaid expenses and other current assets | 538 | 514 | ||||||
Total current assets | 18,200 | 14,990 | ||||||
Long-term investments | 13,311 | 13,366 | ||||||
Property, equipment and capitalized software, net of accumulated depreciation and amortization of $2,738 and $2,363 | 2,140 | 2,181 | ||||||
Goodwill | 20,727 | 20,088 | ||||||
Other intangible assets, net of accumulated amortization of $1,038 and $803 | 2,381 | 2,329 | ||||||
Other assets | 2,286 | 2,861 | ||||||
TOTAL ASSETS | $ | 59,045 | $ | 55,815 | ||||
LIABILITIES AND SHAREHOLDERS' EQUITY | ||||||||
Current liabilities: | ||||||||
Medical costs payable | $ | 9,362 | $ | 8,664 | ||||
Accounts payable and accrued liabilities | 6,283 | 5,685 | ||||||
Other policy liabilities | 3,137 | 2,823 | ||||||
Commercial paper and current maturities of long-term debt | 2,164 | 1,456 | ||||||
Unearned revenues | 1,217 | 1,133 | ||||||
Total current liabilities | 22,163 | 19,761 | ||||||
Long-term debt, less current maturities | 9,009 | 11,338 | ||||||
Future policy benefits | 2,325 | 2,286 | ||||||
Other liabilities | 1,942 | 1,650 | ||||||
Total liabilities | 35,439 | 35,035 | ||||||
Commitments and contingencies (Note 14) | ||||||||
Shareholders' equity: | ||||||||
Preferred stock, $0.001 par value - 10 shares authorized; no shares issued or outstanding | - | - | ||||||
Common stock, $0.01 par value - 3,000 shares authorized; 1,147 and 1,201 issued and outstanding | 11 | 12 | ||||||
Additional paid-in capital | - | 38 | ||||||
Retained earnings | 23,342 | 20,782 | ||||||
Accumulated other comprehensive income (loss): | ||||||||
Net unrealized gains (losses) on investments, net of tax effects | 277 | (30 | ) | |||||
Foreign currency translation losses | (24 | ) | (22 | ) | ||||
Total shareholders' equity | 23,606 | 20,780 | ||||||
TOTAL LIABILITIES AND SHAREHOLDERS' EQUITY | $ | 59,045 | $ | 55,815 | ||||
See Notes to the Consolidated Financial Statements.
53
UnitedHealth Group
Consolidated Statements of Operations
| For the Year Ended December 31, | ||||||||||||
(in millions, except per share data) | 2009 | 2008 | 2007 | |||||||||
REVENUES: | ||||||||||||
Premiums | $ | 79,315 | $ | 73,608 | $ | 68,781 | ||||||
Services | 5,306 | 5,152 | 4,608 | |||||||||
Products | 1,925 | 1,655 | 898 | |||||||||
Investment and other income | 592 | 771 | 1,144 | |||||||||
Total revenues | 87,138 | 81,186 | 75,431 | |||||||||
OPERATING COSTS: | ||||||||||||
Medical costs | 65,289 | 60,359 | 55,435 | |||||||||
Operating costs | 12,734 | 13,103 | 10,583 | |||||||||
Cost of products sold | 1,765 | 1,480 | 768 | |||||||||
Depreciation and amortization | 991 | 981 | 796 | |||||||||
Total operating costs | 80,779 | 75,923 | 67,582 | |||||||||
EARNINGS FROM OPERATIONS | 6,359 | 5,263 | 7,849 | |||||||||
Interest expense | (551 | ) | (639 | ) | (544 | ) | ||||||
EARNINGS BEFORE INCOME TAXES | 5,808 | 4,624 | 7,305 | |||||||||
Provision for income taxes | (1,986 | ) | (1,647 | ) | (2,651 | ) | ||||||
NET EARNINGS | $ | 3,822 | $ | 2,977 | $ | 4,654 | ||||||
BASIC NET EARNINGS PER COMMON SHARE | $ | 3.27 | $ | 2.45 | $ | 3.55 | ||||||
DILUTED NET EARNINGS PER COMMON SHARE | $ | 3.24 | $ | 2.40 | $ | 3.42 | ||||||
BASIC WEIGHTED-AVERAGE NUMBER OF COMMON SHARES OUTSTANDING | 1,168 | 1,214 | 1,312 | |||||||||
DILUTIVE EFFECT OF COMMON STOCK EQUIVALENTS | 11 | 27 | 49 | |||||||||
DILUTED WEIGHTED-AVERAGE NUMBER OF COMMON SHARES OUTSTANDING | 1,179 | 1,241 | 1,361 | |||||||||
ANTI-DILUTIVE SHARES EXCLUDED FROM THE CALCULATION OF DILUTIVE EFFECT OF COMMON STOCK EQUIVALENTS | 107 | 90 | 38 | |||||||||
See Notes to the Consolidated Financial Statements.
54
UnitedHealth Group
Consolidated Statements of Changes in Shareholders' Equity
| Common Stock | Additional Paid-In Capital | Retained Earnings | Accumulated Other Comprehensive Income (Loss) | Total Shareholders' Equity | |||||||||||||||||||
(in millions) | Shares | Amount | |||||||||||||||||||||
Balance at January 1, 2007 | 1,345 | $ | 13 | $ | 6,406 | $ | 14,376 | $ | 15 | $ | 20,810 | ||||||||||||
Net earnings | - | - | - | 4,654 | - | 4,654 | |||||||||||||||||
Unrealized holding gains on investment securities during the period, net of tax expense of $60 | - | - | - | - | 107 | 107 | |||||||||||||||||
Reclassification adjustment for net realized gains included in net earnings, net of tax expense of $14 | - | - | - | - | (24 | ) | (24 | ) | |||||||||||||||
Comprehensive income | 4,737 | ||||||||||||||||||||||
Issuances of common stock, and related tax benefits | 33 | 1 | 590 | - | - | 591 | |||||||||||||||||
Common stock repurchases | (125 | ) | (1 | ) | (6,598 | ) | - | - | (6,599 | ) | |||||||||||||
Conversion of convertible debt | - | - | 24 | - | - | 24 | |||||||||||||||||
Share-based compensation, and related tax benefits | - | - | 602 | - | - | 602 | |||||||||||||||||
Adjustment to adopt FIN 48 | - | - | (1 | ) | (61 | ) | - | (62 | ) | ||||||||||||||
Common stock dividend ($0.03 per share) | - | - | - | (40 | ) | - | (40 | ) | |||||||||||||||
Balance at December 31, 2007 | 1,253 | $ | 13 | $ | 1,023 | $ | 18,929 | $ | 98 | $ | 20,063 | ||||||||||||
Net earnings | - | - | - | 2,977 | - | 2,977 | |||||||||||||||||
Unrealized holding losses on investment securities during the period, net of tax benefit of $76 | - | - | - | - | (132 | ) | (132 | ) | |||||||||||||||
Reclassification adjustment for net realized losses included in net earnings, net of tax benefit of $2 | - | - | - | - | 4 | 4 | |||||||||||||||||
Foreign currency translation loss | - | - | - | - | (22 | ) | (22 | ) | |||||||||||||||
Comprehensive income | 2,827 | ||||||||||||||||||||||
Issuances of common stock, and related tax benefits | 20 | - | 272 | - | - | 272 | |||||||||||||||||
Common stock repurchases | (72 | ) | (1 | ) | (1,596 | ) | (1,087 | ) | - | (2,684 | ) | ||||||||||||
Share-based compensation, and related tax benefits | - | - | 339 | - | - | 339 | |||||||||||||||||
Common stock dividend ($0.03 per share) | - | - | - | (37 | ) | - | (37 | ) | |||||||||||||||
Balance at December 31, 2008 | 1,201 | $ | 12 | $ | 38 | $ | 20,782 | $ | (52 | ) | $ | 20,780 | |||||||||||
Net earnings | - | - | - | 3,822 | - | 3,822 | |||||||||||||||||
Unrealized holding gains on investment securities during the period, net of tax expense of $187 | - | - | - | - | 314 | 314 | |||||||||||||||||
Reclassification adjustment for net realized gains included in net earnings, net of tax expense of $4 | - | - | - | - | (7 | ) | (7 | ) | |||||||||||||||
Foreign currency translation loss | - | - | - | - | (2 | ) | (2 | ) | |||||||||||||||
Comprehensive income | 4,127 | ||||||||||||||||||||||
Issuances of common stock, and related tax benefits | 20 | - | 221 | - | - | 221 | |||||||||||||||||
Common stock repurchases | (74 | ) | (1 | ) | (574 | ) | (1,226 | ) | - | (1,801 | ) | ||||||||||||
Share-based compensation, and related tax benefits | - | - | 315 | - | - | 315 | |||||||||||||||||
Common stock dividend ($0.03 per share) | - | - | - | (36 | ) | - | (36 | ) | |||||||||||||||
Balance at December 31, 2009 | 1,147 | $ | 11 | $ | - | $ | 23,342 | $ | 253 | $ | 23,606 | ||||||||||||
See Notes to the Consolidated Financial Statements.
55
UnitedHealth Group
Consolidated Statements of Cash Flows
| For the Year Ended December 31, | ||||||||||||
(in millions) | 2009 | 2008 | 2007 | |||||||||
OPERATING ACTIVITIES | ||||||||||||
Net earnings | $ | 3,822 | $ | 2,977 | $ | 4,654 | ||||||
Noncash items: | ||||||||||||
Depreciation and amortization | 991 | 981 | 796 | |||||||||
Deferred income taxes | (16 | ) | (166 | ) | 86 | |||||||
Share-based compensation | 334 | 305 | 505 | |||||||||
Other | 23 | (122 | ) | (213 | ) | |||||||
Net change in other operating items, net of effects from acquisitions and changes in AARP balances: | ||||||||||||
Accounts receivable | 100 | (219 | ) | (194 | ) | |||||||
Other assets | (250 | ) | (48 | ) | (386 | ) | ||||||
Medical costs payable | 424 | (41 | ) | 149 | ||||||||
Accounts payable and other liabilities | 99 | 708 | 269 | |||||||||
Other policy liabilities | 104 | (170 | ) | 188 | ||||||||
Unearned revenues | (6 | ) | 33 | 23 | ||||||||
Cash flows from operating activities | 5,625 | 4,238 | 5,877 | |||||||||
INVESTING ACTIVITIES | ||||||||||||
Cash paid for acquisitions, net of cash assumed | (486 | ) | (4,012 | ) | (270 | ) | ||||||
Cash received from disposition | - | 199 | 8 | |||||||||
Purchases of property, equipment and capitalized software | (739 | ) | (791 | ) | (871 | ) | ||||||
Proceeds from disposal of property, equipment and capitalized software | - | 185 | - | |||||||||
Purchases of investments | (6,466 | ) | (9,251 | ) | (6,379 | ) | ||||||
Sales of investments | 4,040 | 5,568 | 1,271 | |||||||||
Maturities of investments | 2,675 | 3,030 | 2,094 | |||||||||
Cash flows used for investing activities | (976 | ) | (5,072 | ) | (4,147 | ) | ||||||
FINANCING ACTIVITIES | ||||||||||||
(Repayments of) proceeds from commercial paper, net | (99 | ) | (1,346 | ) | 947 | |||||||
Proceeds from issuance of long-term debt | - | 2,981 | 3,582 | |||||||||
Payments for retirement of long-term debt | (1,350 | ) | (500 | ) | (950 | ) | ||||||
Proceeds from interest rate swap termination | 513 | - | - | |||||||||
Common stock repurchases | (1,801 | ) | (2,684 | ) | (6,599 | ) | ||||||
Proceeds from common stock issuances | 282 | 299 | 712 | |||||||||
Share-based compensation excess tax benefit | 38 | 62 | 303 | |||||||||
Customer funds administered | 204 | (461 | ) | (1,110 | ) | |||||||
Dividends paid | (36 | ) | (37 | ) | (40 | ) | ||||||
Checks outstanding | 22 | 1,224 | - | |||||||||
Other | (48 | ) | (143 | ) | (30 | ) | ||||||
Cash flows used for financing activities | (2,275 | ) | (605 | ) | (3,185 | ) | ||||||
INCREASE (DECREASE) IN CASH AND CASH EQUIVALENTS | 2,374 | (1,439 | ) | (1,455 | ) | |||||||
CASH AND CASH EQUIVALENTS, BEGINNING OF PERIOD | 7,426 | 8,865 | 10,320 | |||||||||
CASH AND CASH EQUIVALENTS, END OF PERIOD | $ | 9,800 | $ | 7,426 | $ | 8,865 | ||||||
Supplemental cash flow disclosures | ||||||||||||
Cash paid for interest | $ | 527 | $ | 621 | $ | 553 | ||||||
Cash paid for income taxes | $ | 2,048 | $ | 1,882 | $ | 2,277 | ||||||
See Notes to the Consolidated Financial Statements.
56
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
1. Description of Business
UnitedHealth Group Incorporated (also referred to as "UnitedHealth Group" and "the Company") is a diversified health and well-being company dedicated to making health care work better. The Company emphasizes enhancing the performance of the health system and improving the overall health and well-being of the people it serves and their communities. The Company helps people get the care they need at an affordable cost; supports the physician/patient relationship; and empowers people with the information, guidance and tools they need to make personal health choices and decisions.
The Company's primary focus is on improving the health care system by simplifying the administrative components of health care delivery, promoting evidence-based medicine as the standard for care, and providing relevant, actionable data that physicians, health care professionals, consumers, employers and other participants in health care can use to make better, more informed decisions.
Through its diversified family of businesses, the Company leverages core competencies in advanced technology-based transactional capabilities; health care data, knowledge and information; and health care resource organization and care facilitation to improve access to health and well-being services, simplify the health care experience, promote quality and make health care more affordable.
2. Basis of Presentation and Summary of Significant Accounting Policies
Basis of Presentation
The Company has prepared the Consolidated Financial Statements according to U.S. Generally Accepted Accounting Principles (GAAP) and has included the accounts of UnitedHealth Group and its subsidiaries. The Company has eliminated intercompany balances and transactions.
The Company has evaluated subsequent events through February 10, 2010, the date this Form 10-K was filed with the SEC. Other than the debt tender that is discussed in Note 9 of Notes to the Consolidated Financial Statements and the change to the Company's share repurchase program discussed in Note 11 of Notes to the Consolidated Financial Statements, no material subsequent events have occurred since December 31, 2009 that required recognition or disclosure in these financial statements.
Use of Estimates
These Consolidated Financial Statements include certain amounts based on the Company's best estimates and judgments. The Company's most significant estimates relate to medical costs, medical costs payable, revenues, goodwill, other intangible assets, investments, income taxes and contingent liabilities. These estimates require the application of complex assumptions and judgments, often because they involve matters that are inherently uncertain and will likely change in subsequent periods. The impact of any changes in estimates is included in earnings in the period in which the estimate is adjusted.
Revenues
Premium revenues are primarily derived from risk-based health insurance arrangements in which the premium is fixed, typically for a one-year period, and the Company assumes the economic risk of funding its customers' health care and related administrative costs. The Company recognizes premium revenues in the period in which eligible individuals are entitled to receive health care benefits. The Company records health care premium payments received from its customers in advance of the service period as unearned revenues.
57
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
Centers for Medicare and Medicaid Services (CMS) deploys a risk adjustment model that apportions premiums paid to all health plans according to health severity and certain demographic factors. The CMS risk adjustment model pays more for members whose medical history indicates they have certain medical conditions. Under this risk adjustment methodology, CMS calculates the risk adjusted premium payment using diagnosis data from hospital inpatient, hospital outpatient and physician treatment settings. The Company and health care providers collect, capture, and submit the necessary and available diagnosis data to CMS within prescribed deadlines. The Company estimates risk adjustment revenues based upon the diagnosis data submitted and expected to be submitted to CMS.
Service revenues consist primarily of fees derived from services performed for customers that self-insure the health care costs of their employees and employees' dependants. Under service fee contracts, the Company recognizes revenue in the period the related services are performed based upon the fee charged to the customer. The customers retain the risk of financing health care costs for their employees and employees' dependants, and the Company administers the payment of customer funds to physicians and other health care professionals from customer-funded bank accounts. Since the Company has neither the obligation for funding the health care costs, nor the responsibility for providing the medical care, the Company does not recognize premium revenue and medical costs for these contracts in its Consolidated Financial Statements.
For both risk-based and fee-based customer arrangements, the Company provides coordination and facilitation of medical services; transaction processing; customer, consumer and care professional services; and access to contracted networks of physicians, hospitals and other health care professionals.
Through the Company's Prescription Solutions pharmacy benefits management (PBM) business, revenues are derived from products sold through a contracted network of retail pharmacies, and from administrative services, including claims processing and formulary design and management. Product revenues include ingredient costs (net of rebates), a negotiated dispensing fee and customer co-payments for drugs dispensed through the Company's mail-service pharmacy. In retail pharmacy transactions, revenues recognized always exclude the member's applicable co-payment. Product revenues are recognized upon sale or shipment based on contract terms. Service revenues are recognized when the prescription claim is adjudicated. The Company has entered into retail service contracts in which it is primarily obligated to pay its network pharmacy providers for benefits provided to their customers regardless if the Company is paid. The Company is also involved in establishing the prices charged by retail pharmacies, determining which drugs will be included in formulary listings and selecting which retail pharmacies will be included in the network offered to plan sponsors' members. As a result, revenues are reported on a gross basis. Product revenues also include sales of Ingenix publishing and software products that are recognized as revenue upon shipment.
Medical Costs and Medical Costs Payable
Medical costs and medical costs payable include estimates of the Company's obligations for medical care services that have been rendered on behalf of insured consumers but for which the Company has either not yet received or processed claims, and for liabilities for physician, hospital and other medical cost disputes. The Company develops estimates for medical costs incurred but not reported using an actuarial process that is consistently applied, centrally controlled and automated. The actuarial models consider factors such as time from date of service to claim receipt, claim backlogs, care professional contract rate changes, medical care consumption and other medical cost trends. The Company estimates liabilities for physician, hospital and other medical cost disputes based upon an analysis of potential outcomes, assuming a combination of litigation and settlement strategies. Each period, the Company re-examines previously established medical costs payable estimates based on actual claim submissions and other changes in facts and circumstances. As the liability estimates recorded in prior periods become more exact, the Company adjusts the amount of the estimates, and
58
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
includes the changes in estimates in medical costs in the period in which the change is identified. In every reporting period, the Company's operating results include the effects of more completely developed medical costs payable estimates associated with previously reported periods.
Cash, Cash Equivalents and Investments
Cash and cash equivalents are highly liquid investments that have an original maturity of three months or less. The fair value of cash and cash equivalents approximates their carrying value because of the short maturity of the instruments.
The Company had checks outstanding in excess of bank deposits of $1.2 billion as of both December 31, 2009 and 2008, which were classified as Accounts Payable and Accrued Liabilities in the Consolidated Balance Sheets and have been reflected as Checks Outstanding within financing activities in the Consolidated Statements of Cash Flows. During the fourth quarter of 2008, the Company changed its intent with respect to offsetting cash balances, which affected its balances in checks outstanding in excess of bank deposits for certain cash balances. There were no checks outstanding in excess of bank deposits as of December 31, 2007.
Investments with maturities of less than one year are classified as short-term. Because of regulatory requirements, certain investments are included in long-term investments regardless of their maturity date. The Company classifies these investments as held-to-maturity and reports them at amortized cost. Substantially all other investments are classified as available-for-sale and reported at fair value based on quoted market prices, where available.
The Company excludes unrealized gains and losses on investments in available-for-sale securities from earnings and reports them, net of income tax effects, as a separate component of shareholders' equity. The Company evaluates investments for impairment by considering the length of time and extent to which market value has been less than cost, the financial condition and near-term prospects of the issuer as well as specific events or circumstances that may influence the operations of the issuer and the Company's intent to sell the security or the likelihood that it will be required to sell the security before recovery of the entire amortized cost. For debt securities, if the Company intends to either sell or determines that it will be more likely than not be required to sell a security before recovery of the entire amortized cost basis or maturity of the security, the Company recognizes the entire impairment in earnings. If the Company does not intend to sell the debt security and it determines that it will not be more likely than not be required to sell the security but it does not expect to recover the entire amortized cost basis, the impairment is bifurcated into the amount attributed to the credit loss, which is recognized in earnings, and all other causes, which are recognized in other comprehensive income. For equity securities, the Company recognizes impairments in other comprehensive income if it expects to hold the security until fair value increases to at least the security's cost basis and it expects that increase in fair value to occur in a reasonably forecasted period. If the Company intends to sell the equity security or if it believes that recovery of fair value to cost will not occur in a reasonably forecasted period, the Company recognizes the impairment in net earnings. New information and the passage of time can change these judgments. The Company manages its investment portfolio to limit its exposure to any one issuer or market sector, and largely limits its investments to U.S. government and agency securities; state and municipal securities; mortgage-backed securities; and corporate debt obligations, substantially all of investment grade quality. Securities downgraded below policy minimums after purchase will be disposed of in accordance with the investment policy. To calculate realized gains and losses on the sale of investments, the Company uses the specific cost or amortized cost of each investment sold.
Assets Under Management
The Company administers certain aspects of AARP's insurance program (see Note 13 of Notes to the Consolidated Financial Statements). Pursuant to the Company's agreement, AARP assets are managed separately
59
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
from its general investment portfolio and are used to pay costs associated with the AARP program. These assets are invested at the Company's discretion, within investment guidelines approved by AARP. The Company does not guarantee any rates of return on these investments and, upon transfer of the AARP contract to another entity, the Company would transfer cash equal in amount to the fair value of these investments at the date of transfer to that entity. Because the purpose of these assets is to fund the medical costs payable, the rate stabilization fund (RSF) liabilities and other related liabilities associated with the AARP contract, assets under management are classified as current assets, consistent with the classification of these liabilities. Interest earnings and realized investment gains and losses on these assets accrue to the overall benefit of the AARP policyholders through the RSF. Accordingly, they are not included in the Company's earnings.
Other Current Receivables
Other current receivables include amounts due from pharmacy rebates, CMS for Medicare Part D, reinsurance and other miscellaneous amounts due to the Company.
The Company's PBM businesses contract with pharmaceutical manufacturers, some of whom provide rebates based on use of the manufacturers' products by its PBM businesses' affiliated and non-affiliated clients. The Company accrues rebates as they are earned by its clients on a monthly basis based on the terms of the applicable contracts, historical data and current estimates. The PBM businesses bill these rebates to the manufacturers on a monthly or quarterly basis depending on the contractual terms. The PBM businesses record rebates attributable to affiliated clients as a reduction to medical costs. Rebates attributable to non-affiliated clients are accrued as rebates receivable and a reduction of cost of products sold with a corresponding payable for the amounts of the rebates to be remitted to non-affiliated clients in accordance with their contracts and recorded in the Consolidated Statements of Operations as a reduction of Product Revenue. The Company generally receives rebates between two to five months after billing.
For details on the Company's Medicare Part D receivables see "Medicare Part D Pharmacy Benefits Contract" below.
For details on the Company's reinsurance receivable see "Future Policy Benefits and Reinsurance Receivables" below.
Medicare Part D Pharmacy Benefits Contract
The Company serves as a plan sponsor offering Medicare Part D prescription drug insurance coverage under contracts with CMS. Under the Medicare Part D program, there are six separate elements of payment received by the Company during the plan year. These payment elements are as follows:
| • | CMS Premium. CMS pays a fixed monthly premium per member to the Company for the entire plan year. |
| • | Member Premium. Additionally, certain members pay a fixed monthly premium to the Company for the entire plan year. |
| • | Low-Income Premium Subsidy. For qualifying low-income members, CMS pays some or all of the member's monthly premiums to the Company on the member's behalf. |
| • | Catastrophic Reinsurance Subsidy . CMS pays the Company a cost reimbursement estimate monthly to fund the CMS obligation to pay approximately 80% of the costs incurred by individual members in excess of the individual annual out-of-pocket maximum. A settlement is made with CMS based on actual cost experience, after the end of the plan year. |
60
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
| • | Low-Income Member Cost Sharing Subsidy. For qualifying low-income members, CMS pays on the member's behalf some or all of a member's cost sharing amounts, such as deductibles and coinsurance. The cost sharing subsidy is funded by CMS through monthly payments to the Company. The Company administers and pays the subsidized portion of the claims on behalf of CMS, and a settlement payment is made between CMS and the Company based on actual claims and premium experience, after the end of the plan year. |
| • | CMS Risk-Share. Premiums from CMS are subject to risk corridor provisions that compare costs targeted in the Company's annual bids to actual prescription drug costs, limited to actual costs that would have been incurred under the standard coverage as defined by CMS. Variances of more than 5% above or below the original bid submitted by the Company may result in CMS making additional payments to the Company or require the Company to refund to CMS a portion of the premiums it received. The Company estimates and recognizes an adjustment to premium revenues related to the risk corridor payment settlement based upon pharmacy claims experience. The estimate of the settlement associated with these risk corridor provisions requires the Company to consider factors that may not be certain, including member eligibility status differences with CMS. The Company records risk-share adjustments to Premium Revenues in the Consolidated Statements of Operations and Other Policy Liabilities or Other Current Receivables in the Consolidated Balance Sheets. |
The CMS Premium, the Member Premium, and the Low-Income Premium Subsidy represent payments for the Company's insurance risk coverage under the Medicare Part D program and therefore are recorded as Premium Revenues in the Consolidated Statements of Operations. Premium revenues are recognized ratably over the period in which eligible individuals are entitled to receive prescription drug benefits. The Company records premium payments received in advance of the applicable service period in Unearned Revenues in the Consolidated Balance Sheets.
The Catastrophic Reinsurance Subsidy and the Low-Income Member Cost Sharing Subsidy represent cost reimbursements under the Medicare Part D program. The Company is fully reimbursed by CMS for costs incurred for these contract elements and, accordingly, there is no insurance risk to the Company. Amounts received for these subsidies are not reflected as premium revenues, but rather are accounted for as deposits. As of December 31, 2009 and 2008, the amounts received for these subsidies were insufficient to cover the costs incurred for these contract elements; therefore, the Company recorded a receivable in Other Current Receivables in the Consolidated Balance Sheets. Related cash flows are presented as Customer Funds Administered within financing activities in the Consolidated Statements of Cash Flows.
Pharmacy benefit costs and administrative costs under the contract are expensed as incurred and are recognized in Medical Costs and Operating Costs, respectively, in the Consolidated Statements of Operations.
The final 2009 risk-share amount is expected to be settled during the second half of 2010, and is subject to the reconciliation process with CMS.
The Consolidated Balance Sheets include the following amounts associated with the Medicare Part D program:
| December 31, 2009 | December 31, 2008 | |||||||||||
(in millions) | CMS Subsidies (a) | Risk-Share | CMS Subsidies (a) | Risk-Share | ||||||||
Other current receivables | $ | 271 | $ | - | $ | 349 | $ | 19 | ||||
Other policy liabilities | - | 268 | - | - | ||||||||
| (a) | Includes the Catastrophic Reinsurance Subsidy and the Low-Income Member Cost Sharing Subsidy. |
61
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
As of January 1, 2010, certain changes were made to the Medicare Part D coverage by CMS, including:
| • | The initial coverage limit increased to $2,830 from $2,700 in 2009. |
| • | The catastrophic coverage begins at $6,440 as compared to $6,154 in 2009. |
| • | The annual out-of-pocket maximum increased to $4,550 from $4,350 in 2009. |
Property, Equipment and Capitalized Software
Property, equipment and capitalized software are stated at cost, net of accumulated depreciation and amortization. Capitalized software consists of certain costs incurred in the development of internal-use software, including external direct costs of materials and services and payroll costs of employees devoted to specific software development. The Company reviews property, equipment and capitalized software for events or changes in circumstances that would indicate that we might not recover their carrying value. If the Company determines that an asset may not be recoverable, an impairment charge is recorded.
The Company calculates depreciation and amortization using the straight-line method over the estimated useful lives of the assets. The useful lives for property, equipment and capitalized software are:
Furniture, fixtures and equipment | 3 to 7 years | |
Buildings | 35 to 40 years | |
Leasehold improvements | Shorter of useful life or remaining lease term | |
Capitalized software | 3 to 5 years |
Goodwill
Goodwill represents the amount of the purchase price in excess of the fair values assigned to the underlying identifiable net assets of acquired businesses. Goodwill is not amortized, but is subject to an annual impairment test. Tests are performed more frequently if events occur or circumstances change that would more likely than not reduce the fair value of the reporting unit below its carrying amount. To determine whether goodwill is impaired, the Company performs a two-step impairment test. In the first step of the test, the fair values of the reporting units are compared to their aggregate carrying values, including goodwill. If the fair value of the reporting unit is greater than its carrying amount, goodwill is not impaired and no further testing is required. If the fair value of the reporting unit is less than its carrying amount, the Company would proceed to step two of the test. In step two of the test, the implied fair value of the goodwill of the reporting unit is determined by a hypothetical allocation of the fair value calculated in step one to all of the assets and liabilities of that reporting unit (including any recognized and unrecognized intangible assets) as if the reporting unit had been acquired in a business combination and the fair value was reflective of the price paid to acquire the reporting unit. The implied fair value of goodwill is the excess, if any, of the calculated fair value after hypothetical allocation to the reporting unit's assets and liabilities. If the implied fair value of the goodwill is greater than the carrying amount of the goodwill at the analysis date, goodwill is not impaired and the analysis is complete. If the implied fair value of the goodwill is less than the carrying value of goodwill at the analysis date, goodwill is deemed impaired by the amount of that variance.
The Company calculates the estimated fair value of our reporting units using discounted cash flows. To determine fair values the Company must make assumptions about a wide variety of internal and external factors. Significant assumptions used in the impairment analysis include financial projections of free cash flow (includes significant assumptions about operations, capital requirements and income taxes), long-term growth rates for determining terminal value, and discount rates. Where available and appropriate, comparative market multiples are used to corroborate the results of our discounted cash flow test.
62
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The Company completed its annual assessment of goodwill as of January 1, 2010 and determined that no impairment existed as of December 31, 2009. Although the Company believes that the financial projections used are reasonable and appropriate for all of its reporting units, there is uncertainty inherent in those projections. That uncertainty is increased by potential health care reforms, as any passed legislation may significantly change the forecasts and long-term growth rate assumptions for some or all of its reporting units.
Intangible assets
Finite lived intangible assets are acquired in a business combination and are assets that represent future expected benefits but lack physical substance (e.g., customer lists and trademarks). The Company does not have material holdings of indefinite lived intangible assets. Intangible assets are amortized over their expected useful lives and are subject to impairment tests when events or circumstances indicate that a finite lived intangible asset's (or asset group's) carrying value may exceed its estimated fair value. If the carrying value exceeds its estimated fair value, an impairment would be recorded.
The Company calculates the estimated fair value of finite lived intangible assets using undiscounted cash flows that are expected to result from the use of the intangible asset or group of assets. The Company considers many factors, including estimated future utility to estimate cash flows. There were no material impairments of finite lived intangible assets during the current year.
Other Policy Liabilities
Other policy liabilities include the RSF associated with the AARP program (see Note 13 of Notes to the Consolidated Financial Statements), health savings account deposits, deposits under the Medicare Part D program (see "Medicare Part D Pharmacy Benefits Contract" above), and the current portion of future policy benefits. Customer balances represent excess customer payments and deposit accounts under experience-rated contracts. At the customer's option, these balances may be refunded or used to pay future premiums or claims under eligible contracts.
Income Taxes
Deferred income tax assets and liabilities are recognized for the differences between the financial and income tax reporting bases of assets and liabilities based on enacted tax rates and laws. The deferred income tax provision or benefit generally reflects the net change in deferred income tax assets and liabilities during the year, excluding any deferred income tax assets and liabilities of acquired businesses. The current income tax provision reflects the tax consequences of revenues and expenses currently taxable or deductible on various income tax returns for the year reported.
Future Policy Benefits and Reinsurance Receivables
Future policy benefits represent account balances that accrue to the benefit of the policyholders, excluding surrender charges, for universal life and investment annuity products and health policies sold to individuals for which some of the premium received in the earlier years is intended to pay benefits to be incurred in future years. As a result of the 2005 sale of the life and annuity business within the Company's Golden Rule Financial Corporation (Golden Rule) subsidiary under an indemnity reinsurance arrangement, the Company has maintained a liability associated with the reinsured contracts, as it remains primarily liable to the policyholders, and has recorded a corresponding reinsurance receivable due from the purchaser. As of December 31, 2009, the Company had an aggregate $2.0 billion reinsurance receivable, of which $139 million was recorded in Other Current Receivables and $1.9 billion was recorded in Other Assets in the Consolidated Balance Sheets. As of
63
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
December 31, 2008, the Company had an aggregate $2.0 billion reinsurance receivable, of which $154 million was recorded in Other Current Receivables and $1.9 billion was recorded in Other Assets in the Consolidated Balance Sheets. The Company evaluates the financial condition of the reinsurer and only records the reinsurance receivable to the extent of probable recovery.
Policy Acquisition Costs
The Company's commercial health insurance contracts typically have a one-year term and may be cancelled by the customer with at least 31 days notice. Costs related to the acquisition and renewal of commercial customer contracts are charged to expense as incurred.
Share-Based Compensation
Share-based compensation expense is measured at the grant date based on the fair values of the awards and is recognized as expense over the period in which the share-based compensation vests.
Net Earnings Per Common Share
The Company computes basic net earnings per common share by dividing net earnings by the weighted-average number of common shares outstanding during the period. The Company determines diluted net earnings per common share using the weighted-average number of common shares outstanding during the period, adjusted for potentially dilutive shares associated with stock options and restricted stock, using the treasury stock method. The treasury stock method assumes exercise of stock options and vesting of restricted stock, with the assumed proceeds used to purchase common stock at the average market price for the period. The difference between the number of shares assumed issued and number of shares assumed purchased represents the dilutive shares.
Recent Accounting Standards
Recently Adopted Accounting Standards. In June 2009, the Financial Accounting Standards Board (FASB) issued Statement of Financial Accounting Standards (FAS) No. 168, "The FASB Accounting Standards Codification and the Hierarchy of Generally Accepted Accounting Principles - a replacement of FAS 162." The new standard establishes only two levels of U.S. GAAP, authoritative and nonauthoritative. The FASB Accounting Standards Codification (ASC) became the single source of authoritative, nongovernmental U.S. GAAP, except for rules and interpretive releases of the SEC, which will continue to be sources of authoritative U.S. GAAP for SEC registrants. All other non-grandfathered, non-SEC accounting literature not included in the ASC became nonauthoritative upon adoption. The new guidance became effective for the Company's third quarter of 2009. Since the new standard did not change U.S. GAAP, there was no change to the Company's Consolidated Financial Statements other than to update all references to U.S. GAAP to be in conformity with the ASC.
The Company adopted the provisions of ASC Topic No. 820, "Fair Value Measurements and Disclosures" (ASC 820) as of January 1, 2008 for fair value measurements of certain financial assets and liabilities and for non-financial assets and liabilities measured at fair value on at least an annual basis. The provisions were adopted for non-financial assets and liabilities not measured at fair value on at least an annual basis as of January 1, 2009. These provisions define fair value, establish a framework for measuring fair value and expand disclosure requirements. The adoption did not have a material impact on the Consolidated Financial Statements.
In December 2007, the FASB issued guidance codified into ASC Topic No. 805, "Business Combinations," which replaced previous business combination accounting guidance. The new guidance revises how an acquirer
64
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
recognizes and measures in its financial statements the identifiable assets acquired, the liabilities, any noncontrolling interest in the acquiree and the goodwill acquired. The guidance as amended includes recognition provisions for assets acquired and liabilities assumed that arise from contingencies and the treatment of contingent purchase price. It also requires additional disclosure requirements intended to enable users to evaluate the nature and financial effects of the business combination. The Company adopted the new guidance on January 1, 2009, and applied the provisions prospectively to all new acquisitions closing on or after that date. The adoption did not have a material impact on the Consolidated Financial Statements.
Recently Issued Accounting Standards. In October 2009, the FASB issued Accounting Standards Update (ASU) No. 2009-13, "Multiple-Deliverable Revenue Arrangements" (ASU 2009-13). This update removes the criterion that entities must use objective and reliable evidence of fair value in separately accounting for deliverables and provides entities with a hierarchy of evidence that must be considered when allocating arrangement consideration. The new guidance also requires entities to allocate arrangement consideration to the separate units of accounting based on the deliverables' relative selling price. The provisions will be effective for revenue arrangements entered into or materially modified in the Company's fiscal year 2011 and must be applied prospectively. The Company is currently evaluating the impact of the provisions of ASU 2009-13.
The Company has determined that all other recently issued accounting standards will not have a material impact on its Consolidated Financial Statements, or do not apply to its operations.
3. Acquisitions
On June 1, 2009, all of the outstanding shares of AIM Healthcare Services, Inc. (AIM) were acquired for approximately $440 million in cash. AIM is a leading provider of payment accuracy solutions for health care payer and hospital clients in all 50 states. On a preliminary basis, the total consideration paid exceeded the estimated fair value of the net tangible assets acquired by $425 million, of which $166 million has been allocated to finite-lived intangible assets and $259 million to goodwill. The allocation is pending completion of a valuation analysis. The acquired goodwill is deductible for income tax purposes. The results of operations and financial condition of AIM have been included in the Company's consolidated results and the results of the Ingenix reporting segment since the acquisition date. The pro forma effects of this acquisition on the Company's Consolidated Financial Statements were not material.
On May 30, 2008, the Company acquired all the outstanding shares of Unison Health Plans (Unison) for approximately $930 million in cash. Unison provides government-sponsored health plan coverage to people in Pennsylvania, Ohio, Tennessee, Delaware, South Carolina and Washington, D.C. through a network of independent health care professionals. The total consideration paid exceeded the estimated fair value of the net tangible assets acquired by $806 million, of which $89 million has been allocated to finite-lived intangible assets and $717 million to goodwill. The acquired goodwill is not deductible for income tax purposes. The results of operations and financial condition of Unison have been included in the Company's consolidated results and the results of the Health Benefits reporting segment since the acquisition date. The pro forma effects of this acquisition on the Company's Consolidated Financial Statements were not material.
On February 25, 2008, the Company acquired all of the outstanding shares of Sierra Health Services, Inc. (Sierra), a diversified health care services company based in Las Vegas, Nevada, for approximately $2.6 billion in cash, representing a price of $43.50 per share of Sierra common stock. The total consideration paid exceeded the estimated fair value of the net tangible assets acquired by $2.5 billion. Based on management's consideration of fair value, which included completion of a valuation analysis, $500 million has been allocated to finite-lived intangible assets and $2.0 billion to goodwill. The acquired goodwill is not deductible for income tax purposes.
65
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The U.S. Department of Justice approved the acquisition conditioned upon the divestiture of the Company's individual Medicare Advantage HMO plans in Clark and Nye Counties, Nevada, which represented approximately 30,000 members. The divestiture was completed on April 30, 2008. The Company received proceeds of $185 million for this transaction, which were recorded as a reduction to Operating Costs. Group Medicare Advantage plans offered through commercial contracts were excluded from the divestiture. Also, the Company retained Sierra's Medicare Advantage HMO plans in Nevada. The results of operations and financial condition of Sierra have been included in the Company's consolidated results and the results of the Health Benefits, OptumHealth and Prescription Solutions reporting segments since the acquisition date. The pro forma effects of this acquisition on the Company's Consolidated Financial Statements were not material.
On January 10, 2008, the Company acquired all of the outstanding shares of Fiserv Health, Inc. (Fiserv Health), a subsidiary of Fiserv, Inc., for approximately $740 million in cash. Fiserv Health is a leading administrator of medical benefits and also provides care facilitation services, specialty health solutions and PBM services. The total consideration paid exceeded the estimated fair value of the net tangible assets acquired by $752 million, of which $253 million has been allocated to finite-lived intangible assets and $499 million to goodwill. The acquired goodwill is deductible for income tax purposes. The results of operations and financial condition of Fiserv Health have been included in the Company's consolidated results and the results of the Health Benefits, OptumHealth, Ingenix and Prescription Solutions reporting segments since the acquisition date. The pro forma effects of this acquisition on the Company's Consolidated Financial Statements were not material.
The finite-lived intangible assets and related weighted-average useful lives, by acquisition, as of acquisition date, consisted of the following:
| AIM | Unison | Sierra | Fiserv | |||||||||||||||||
(in millions, except years) | Fair Value | Weighted- Average Useful Life | Fair Value | Weighted- Average Useful Life | Fair Value | Weighted- Average Useful Life | Fair Value | Weighted- Average Useful Life | ||||||||||||
Customer Contracts and Membership Lists | $ | 146 | 14 years | $ | 41 | 6 years | $ | 443 | 14 years | $ | 252 | 12 years | ||||||||
Trademarks | 3 | 15 years | 32 | 20 years | 56 | 20 years | 1 | 3 years | ||||||||||||
Physician and Hospital Networks | 17 | 5 years | 16 | 20 years | 1 | 15 years | n/a | n/a | ||||||||||||
Total Acquired Finite-Lived Intangible Assets | $ | 166 | 11 years | $ | 89 | 9 years | $ | 500 | 14 years | $ | 253 | 12 years | ||||||||
For the years ended December 31, 2009, 2008 and 2007, aggregate consideration paid, net of cash assumed for smaller acquisitions was $95 million, $94 million and $262 million, respectively. These acquisitions were not material to the Company's Consolidated Financial Statements.
66
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
4. Investments
The amortized cost, gross unrealized gains and losses, and fair value of investments, by type, were as follows:
(in millions) | Amortized Cost | Gross Unrealized Gains | Gross Unrealized Losses | Fair Value | |||||||||
December 31, 2009 | |||||||||||||
Debt securities - available-for-sale: | |||||||||||||
U.S. government and agency obligations | $ | 1,566 | $ | 12 | $ | (11 | ) | $ | 1,567 | ||||
State and municipal obligations | 6,080 | 248 | (11 | ) | 6,317 | ||||||||
Corporate obligations | 3,278 | 149 | (6 | ) | 3,421 | ||||||||
U.S. agency mortgage-backed securities | 1,870 | 64 | (3 | ) | 1,931 | ||||||||
Non-U.S. agency mortgage-backed securities | 535 | 8 | (5 | ) | 538 | ||||||||
Total debt securities - available-for-sale | 13,329 | 481 | (36 | ) | 13,774 | ||||||||
Equity securities - available-for-sale | 579 | 12 | (14 | ) | 577 | ||||||||
Debt securities - held-to-maturity: | |||||||||||||
U.S. government and agency obligations | 158 | 4 | - | 162 | |||||||||
State and municipal obligations | 17 | - | - | 17 | |||||||||
Corporate obligations | 24 | - | - | 24 | |||||||||
Total debt securities-held-to-maturity | 199 | 4 | - | 203 | |||||||||
Total investments | $ | 14,107 | $ | 497 | $ | (50 | ) | $ | 14,554 | ||||
December 31, 2008 | |||||||||||||
Debt securities - available-for-sale: | |||||||||||||
U.S. government and agency obligations | $ | 1,276 | $ | 65 | $ | (2 | ) | $ | 1,339 | ||||
State and municipal obligations | 6,440 | 134 | (90 | ) | 6,484 | ||||||||
Corporate obligations | 2,802 | 33 | (132 | ) | 2,703 | ||||||||
U.S. agency mortgage-backed securities | 2,245 | 62 | - | 2,307 | |||||||||
Non-U.S. agency mortgage-backed securities | 744 | - | (105 | ) | 639 | ||||||||
Total debt securities - available-for-sale | 13,507 | 294 | (329 | ) | 13,472 | ||||||||
Equity securities - available-for-sale | 489 | 8 | (20 | ) | 477 | ||||||||
Debt securities - held-to-maturity: | |||||||||||||
U.S. government and agency obligations | 157 | 10 | - | 167 | |||||||||
State and municipal obligations | 19 | - | - | 19 | |||||||||
Corporate obligations | 24 | - | - | 24 | |||||||||
Total debt securities - held-to-maturity | 200 | 10 | - | 210 | |||||||||
Total investments | $ | 14,196 | $ | 312 | $ | (349 | ) | $ | 14,159 | ||||
Included in the Company's investment portfolio were sub-prime home equity lines of credit with fair values of $9 million and $25 million as of December 31, 2009 and 2008, respectively. Also included were Alt-A securities with fair values of $19 million and $36 million as of December 31, 2009 and 2008, respectively.
67
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The fair value of the Company's mortgage-backed securities by credit rating and non-U.S. agency mortgage-backed securities by origination as of December 31, 2009 were as follows:
(in millions) | AAA | AA | A | BBB | Non-Investment Grade | Total Fair Value | ||||||||||||
2007 | $ | 70 | $ | - | $ | 1 | $ | 8 | $ | 4 | $ | 83 | ||||||
2006 | 130 | 3 | 5 | - | 18 | 156 | ||||||||||||
2005 | 135 | 4 | 2 | 5 | 7 | 153 | ||||||||||||
Pre-2005 | 143 | - | 1 | 1 | 1 | 146 | ||||||||||||
U.S agency mortgage-backed securities | 1,931 | - | - | - | - | 1,931 | ||||||||||||
Total | $ | 2,409 | $ | 7 | $ | 9 | $ | 14 | $ | 30 | $ | 2,469 | ||||||
The amortized cost and fair value of available-for-sale debt securities as of December 31, 2009, by contractual maturity, were as follows:
(in millions) | Amortized Cost | Fair Value | ||||
Due in one year or less | $ | 1,383 | $ | 1,394 | ||
Due after one year through five years | 4,378 | 4,573 | ||||
Due after five years through ten years | 2,886 | 2,989 | ||||
Due after ten years | 2,277 | 2,349 | ||||
U.S. agency mortgage-backed securities | 1,870 | 1,931 | ||||
Non-U.S. agency mortgage-backed securities | 535 | 538 | ||||
Total debt securities - available-for-sale | $ | 13,329 | $ | 13,774 | ||
The amortized cost and fair value of held-to-maturity debt securities as of December 31, 2009, by contractual maturity, were as follows:
(in millions) | Amortized Cost | Fair Value | ||||
Due in one year or less | $ | 60 | $ | 61 | ||
Due after one year through five years | 103 | 105 | ||||
Due after five years through ten years | 26 | 26 | ||||
Due after ten years | 10 | 11 | ||||
Total debt securities - held-to-maturity | $ | 199 | $ | 203 | ||
68
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The fair value of investments with gross unrealized losses by investment type and length of time that individual securities have been in a continuous unrealized loss position were as follows (a):
| Less Than 12 Months | 12 Months or Greater | Total | |||||||||||||||||||
(in millions) | Fair Value | Gross Unrealized Losses | Fair Value | Gross Unrealized Losses | Fair Value | Gross Unrealized Losses | |||||||||||||||
December 31, 2009 | |||||||||||||||||||||
Debt Securities - available-for-sale | |||||||||||||||||||||
U.S. government and agency obligations | $ | 437 | $ | (11 | ) | $ | 4 | $ | - | $ | 441 | $ | (11 | ) | |||||||
State and municipal obligations | 392 | (6 | ) | 100 | (5 | ) | 492 | (11 | ) | ||||||||||||
Corporate obligations | 304 | (3 | ) | 69 | (3 | ) | 373 | (6 | ) | ||||||||||||
U.S. agency mortgage-backed securities | 355 | (3 | ) | 2 | - | 357 | (3 | ) | |||||||||||||
Non-U.S. agency mortgage-backed securities | 134 | (1 | ) | 86 | (4 | ) | 220 | (5 | ) | ||||||||||||
Total debt securities - available-for-sale | $ | 1,622 | $ | (24 | ) | $ | 261 | $ | (12 | ) | $ | 1,883 | $ | (36 | ) | ||||||
Equity securities - available-for-sale | $ | 169 | $ | (13 | ) | $ | 1 | $ | (1 | ) | $ | 170 | $ | (14 | ) | ||||||
December 31, 2008 | |||||||||||||||||||||
Debt securities - available-for-sale | |||||||||||||||||||||
U.S. government and agency obligations | $ | 72 | $ | (2 | ) | $ | - | $ | - | $ | 72 | $ | (2 | ) | |||||||
State and municipal obligations | 1,414 | (65 | ) | 113 | (25 | ) | 1,527 | (90 | ) | ||||||||||||
Corporate obligations | 1,543 | (97 | ) | 179 | (35 | ) | 1,722 | (132 | ) | ||||||||||||
U.S. agency mortgage-backed securities | 17 | - | 5 | - | 22 | - | |||||||||||||||
Non-U.S. agency mortgage-backed securities | 529 | (83 | ) | 88 | (22 | ) | 617 | (105 | ) | ||||||||||||
Total debt securities - available-for-sale | $ | 3,575 | $ | (247 | ) | $ | 385 | $ | (82 | ) | $ | 3,960 | $ | (329 | ) | ||||||
Equity securities - available-for-sale | $ | 195 | $ | (20 | ) | $ | - | $ | - | $ | 195 | $ | (20 | ) | |||||||
| (a) | Debt securities classified as held-to-maturity investments have been excluded from this analysis. These investments are predominantly held in U.S. government or agency obligations. Additionally, the fair values of these investments approximate their amortized cost. |
The Company's mortgage-backed securities in an unrealized loss position by credit rating distribution were as follows:
| December 31, 2009 | December 31, 2008 | |||||||||||||
(in millions) | Fair Value | Gross Unrealized Losses | Fair Value | Gross Unrealized Losses | ||||||||||
AAA | $ | 543 | $ | (6 | ) | $ | 624 | $ | (105 | ) | ||||
AA | 31 | (2 | ) | 1 | - | |||||||||
A | - | - | - | - | ||||||||||
BBB | 1 | - | 13 | - | ||||||||||
Non-investment grade | 2 | - | 1 | - | ||||||||||
Total | $ | 577 | $ | (8 | ) | $ | 639 | $ | (105 | ) | ||||
69
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The unrealized losses as of December 31, 2009 were generated from approximately 1,500 positions out of a total of approximately 12,000 positions. The Company believes that it will collect all principal and interest due on all investments that have an amortized cost in excess of fair value. The unrealized losses on investments in U.S. government and agency obligations, state and municipal obligations and corporate obligations as of December 31, 2009 were primarily caused by interest rate increases and not by unfavorable changes in the credit ratings associated with these securities. The Company evaluates impairment at each reporting period for securities where the fair value of the investment is less than its amortized cost. The contractual cash flows of the U.S. government and agency obligations are guaranteed by either the U.S. government or an agency of the U.S. government. The Company expects that the securities would not be settled at a price less than the amortized cost of the Company's investment. The Company evaluated the underlying credit quality of the issuers and the credit ratings of the state and municipal obligations and the corporate obligations, noting neither a significant deterioration since purchase nor other factors leading to an other-than-temporary impairment (OTTI). The unrealized losses on mortgage-backed securities as of December 31, 2009 were primarily caused by higher interest rates in the marketplace, reflecting the higher perceived risk assigned by fixed-income investors to commercial mortgage-backed securities (CMBS). These unrealized losses represented less than 1% of the total amortized cost of the Company's mortgage-backed security holdings as of December 31, 2009. The Company believes these losses to be temporary. Approximately 94% of the Company's mortgage-backed securities in an unrealized loss position as of December 31, 2009 were rated "AAA" with no known deterioration or other factors leading to an OTTI. As of December 31, 2009, the Company did not have the intent to sell any of the securities in an unrealized loss position.
As of December 31, 2009, the Company's holdings of non-U.S. agency mortgage-backed securities included $10 million of commercial mortgage loans in default. These investments were acquired in the first quarter of 2008 pursuant to an acquisition and were recorded at fair value. They represented less than 1% of the Company's total mortgage-backed security holdings as of December 31, 2009.
A portion of the Company's investments in equity securities and venture capital funds consists of investments held in various public and nonpublic companies concentrated in the areas of health care delivery and related information technologies. Market conditions that affect the value of health care and related technology stocks will likewise impact the value of the Company's equity portfolio. The equity securities and venture capital funds were evaluated for severity and duration of unrealized loss, overall market volatility and other market factors.
Net realized gains, before taxes, were from the following sources:
| Year Ended December 31, | ||||||||||||
(in millions) | 2009 | 2008 | 2007 | |||||||||
Total OTTI | $ | (64 | ) | $ | (121 | ) | $ | (6 | ) | |||
Portion of loss recognized in other comprehensive income | - | n/a | n/a | |||||||||
Net OTTI recognized in earnings | (64 | ) | (121 | ) | (6 | ) | ||||||
Gross realized losses from sales | (41 | ) | (50 | ) | (13 | ) | ||||||
Gross realized gains from sales | 116 | 165 | 57 | |||||||||
Net realized gains (losses) | $ | 11 | $ | (6 | ) | $ | 38 | |||||
For 2009, all of the recorded OTTI resulted from the Company's intent to sell certain impaired securities.
70
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
5. Fair Value
Fair values of available-for-sale debt and equity securities are based on quoted market prices, where available. The Company obtains one price for each security primarily from a third party pricing service (pricing service), which generally uses quoted or other observable inputs for the determination of fair value. The pricing service normally derives the security prices through recently reported trades for identical or similar securities, making adjustments through the reporting date based upon available observable market information. For securities not actively traded, the pricing service may use quoted market prices of comparable instruments or discounted cash flow analyses, incorporating inputs that are currently observable in the markets for similar securities. Inputs that are often used in the valuation methodologies include, but are not limited to, non-binding broker quotes, benchmark yields, credit spreads, default rates and prepayment speeds. As the Company is responsible for the determination of fair value, it performs quarterly analyses on the prices received from the pricing service to determine whether the prices are reasonable estimates of fair value. Specifically, the Company compares the prices received from the pricing service to prices reported by its custodian, its investment consultant and third party investment advisors. Additionally, the Company compares changes in the reported market values and returns to relevant market indices to test the reasonableness of the reported prices. Based on the Company's internal price verification procedures and review of fair value methodology documentation provided by independent pricing services, the Company has not historically adjusted the prices obtained from the pricing service.
In instances in which the inputs used to measure fair value fall into different levels of the fair value hierarchy, the fair value measurement has been determined based on the lowest level input that is significant to the fair value measurement in its entirety. The Company's assessment of the significance of a particular item to the fair value measurement in its entirety requires judgment, including the consideration of inputs specific to the asset.
The fair value hierarchy is as follows:
Level 1 - Quoted (unadjusted) prices for identical assets in active markets.
Level 2 - Other observable inputs, either directly or indirectly, including:
| • | Quoted prices for similar assets in active markets; |
| • | Quoted prices for identical or similar assets in non-active markets (e.g., few transactions, limited information, non-current prices, high variability over time, etc.); |
| • | Inputs other than quoted prices that are observable for the asset (e.g., interest rates, yield curves, volatilities, default rates, etc.); and |
| • | Inputs that are derived principally from or corroborated by other observable market data. |
Level 3 - Unobservable inputs that cannot be corroborated by observable market data.
71
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The following table presents information about the Company's financial assets, excluding AARP, that are measured at fair value on a recurring basis, according to the valuation techniques the Company used to determine their fair values. See Note 13 of Notes to the Consolidated Financial Statements for further detail on AARP.
(in millions, except percentages) | Quoted Prices in Active Markets (Level 1) | Other Observable Inputs (Level 2) | Unobservable Inputs (Level 3) | Total Fair Value | ||||||||||||
December 31, 2009 | ||||||||||||||||
Cash and cash equivalents | $ | 9,135 | $ | 665 | $ | - | $ | 9,800 | ||||||||
Debt securities - available for sale: | ||||||||||||||||
U.S. government and agency obligations | 1,024 | 543 | - | 1,567 | ||||||||||||
State and municipal obligations | - | 6,317 | - | 6,317 | ||||||||||||
Corporate obligations | 18 | 3,293 | 110 | 3,421 | ||||||||||||
U.S. agency mortgage-backed securities | - | 1,931 | - | 1,931 | ||||||||||||
Non-U.S. agency mortgage-backed securities | - | 528 | 10 | 538 | ||||||||||||
Total debt securities - available for sale | 1,042 | 12,612 | 120 | 13,774 | ||||||||||||
Equity securities - available for sale | 262 | 3 | 312 | 577 | ||||||||||||
Total cash, cash equivalents and investments at fair value | $ | 10,439 | $ | 13,280 | $ | 432 | $ | 24,151 | ||||||||
Percentage of total fair value | 43 | % | 55 | % | 2 | % | 100 | % | ||||||||
December 31, 2008 | ||||||||||||||||
Cash and cash equivalents | $ | 6,564 | $ | 862 | $ | - | $ | 7,426 | ||||||||
Debt securities - available-for-sale: | ||||||||||||||||
U.S. government and agency obligations | 800 | 539 | - | 1,339 | ||||||||||||
State and municipal obligations | - | 6,484 | - | 6,484 | ||||||||||||
Corporate obligations | 7 | 2,650 | 46 | 2,703 | ||||||||||||
U.S. agency mortgage-backed securities | - | 2,307 | - | 2,307 | ||||||||||||
Non-U.S. agency mortgage-backed securities | - | 623 | 16 | 639 | ||||||||||||
Total debt securities - available-for-sale | 807 | 12,603 | 62 | 13,472 | ||||||||||||
Equity securities - available-for-sale | 170 | 3 | 304 | 477 | ||||||||||||
Total cash, cash equivalents and investments at fair value | 7,541 | 13,468 | 366 | 21,375 | ||||||||||||
Interest rate swaps | - | 622 | - | 622 | ||||||||||||
Total assets at fair value | $ | 7,541 | $ | 14,090 | $ | 366 | $ | 21,997 | ||||||||
Percentage of total fair value | 34 | % | 64 | % | 2 | % | 100 | % | ||||||||
The following methods and assumptions were used to estimate the fair value of each class of financial instrument:
Cash and Cash Equivalents. The carrying value of cash and cash equivalents approximates fair value as maturities are less than three months. Fair values of cash equivalent instruments that do not trade on a regular basis in active markets are classified as Level 2.
Debt Securities. The estimated fair values of debt securities held as available-for-sale are based on quoted market prices and/or other market data for the same or comparable instruments and transactions in establishing the prices. Fair values of debt securities that do not trade on a regular basis in active markets are classified as Level 2.
72
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
Equity Securities. Equity securities are held as available-for-sale investments. Fair value estimates for Level 1 and Level 2 publicly traded equity securities are based on quoted market prices and/or other market data for the same or comparable instruments and transactions in establishing the prices. The fair values of Level 3 investments in venture capital portfolios are estimated using market modeling approaches that rely heavily on management assumptions and qualitative observations. These investments totaled $282 million as of December 31, 2009. The fair values of the Company's various venture capital investments are computed using limited quantitative and qualitative observations of activity for similar companies in the current market. The key inputs utilized in the Company's market modeling include, as applicable, transactions for comparable companies in similar industries and having similar revenue and growth characteristics; similar preferences in the capital structure; discounted cash flows; liquidation values and milestones established at initial funding; and the assumption that the values of the Company's venture capital investments can be inferred from these inputs. The Company's remaining Level 3 equity securities holdings of $30 million mainly consist of preferred stock for which there is no active market.
Interest Rate Swaps. Fair values of the Company's interest rate swaps were estimated using the terms of the swaps and publicly available market yield curves. Because the swaps were unique and were not actively traded, the fair values were classified as Level 2 estimates. As of December 31, 2009, the Company had no outstanding interest rate swap contracts.
A reconciliation of the beginning and ending balances of assets measured at fair value on a recurring basis using Level 3 inputs is as follows:
| December 31, 2009 | December 31, 2008 | ||||||||||||||||||||||
(in millions) | Debt Securities | Equity Securities | Total | Debt Securities | Equity Securities | Total | |||||||||||||||||
Balance at beginning of period | $ | 62 | $ | 304 | $ | 366 | $ | - | $ | 133 | $ | 133 | |||||||||||
Purchases, net | 64 | 22 | 86 | 14 | 202 | 216 | |||||||||||||||||
Net unrealized gains in accumulated other comprehensive income | - | 7 | 7 | - | 2 | 2 | |||||||||||||||||
Net realized losses in investment and other income | (6 | ) | (21 | ) | (27 | ) | - | (54 | ) | (54 | ) | ||||||||||||
Transfers into Level 3 | - | - | - | 48 | 21 | 69 | |||||||||||||||||
Balance at end of period | $ | 120 | $ | 312 | $ | 432 | $ | 62 | $ | 304 | $ | 366 | |||||||||||
There were no significant fair value adjustments recorded during the year ended December 31, 2009 for non-financial assets and liabilities or financial assets and liabilities that are measured at fair value on a nonrecurring basis. These assets and liabilities are subject to fair value adjustments only in certain circumstances, such as when the Company records impairments.
The table below includes fair values for certain financial instruments for which it is practicable to estimate fair value. The carrying values and fair values of these financial instruments were as follows:
| December 31, 2009 | December 31, 2008 | |||||||||||
(in millions) | Carrying Value | Fair Value | Carrying Value | Fair Value | ||||||||
Assets | ||||||||||||
Debt securities - available-for-sale | $ | 13,774 | $ | 13,774 | $ | 13,472 | $ | 13,472 | ||||
Equity securities - available-for-sale | 577 | 577 | 477 | 477 | ||||||||
Debt securities - held-to-maturity | 199 | 203 | 200 | 210 | ||||||||
AARP program-related investments | 2,114 | 2,114 | 1,941 | 1,941 | ||||||||
Interest rate swaps | - | - | 622 | 622 | ||||||||
Liabilities | ||||||||||||
Senior unsecured notes | 11,173 | 11,043 | 12,693 | 10,941 | ||||||||
73
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
In addition to the previously described methods and assumptions for debt and equity securities and interest rate swaps, the following are the methods and assumptions used to estimate the fair value of the other financial instruments:
AARP Program-related Investments. AARP Program-related investments consist of debt and equity securities held to fund costs associated with the AARP Program (see Note 13 of Notes to the Consolidated Financial Statements). The Company elected to measure the AARP Assets Under Management, of which the investments are a part, at fair value, pursuant to the fair value option. See the preceding discussion regarding the methods and assumptions used to estimate the fair value of debt and equity securities.
Senior Unsecured Notes. The fair values of the senior unsecured notes are estimated based on third-party quoted market prices for the same or similar issues.
The carrying amounts reported in the Consolidated Balance Sheets for cash and cash equivalents, accounts and other current receivables, unearned revenue, accounts payable and accrued liabilities approximate fair value because of their short-term nature. These assets and liabilities are not listed in the table above.
6. Property, Equipment and Capitalized Software
A summary of property, equipment and capitalized software is as follows:
(in millions) | December 31, 2009 | December 31, 2008 | ||||||
Land | $ | 32 | $ | 32 | ||||
Buildings and improvements | 662 | 595 | ||||||
Computer equipment | 1,504 | 1,488 | ||||||
Furniture and fixtures | 235 | 250 | ||||||
Less accumulated depreciation | (1,487 | ) | (1,353 | ) | ||||
Property and equipment, net | 946 | 1,012 | ||||||
Capitalized software | 2,445 | 2,179 | ||||||
Less accumulated amortization | (1,251 | ) | (1,010 | ) | ||||
Capitalized software, net | 1,194 | 1,169 | ||||||
Total property, equipment and capitalized software, net | $ | 2,140 | $ | 2,181 | ||||
Depreciation expense for property and equipment for 2009, 2008 and 2007 was $436 million, $439 million and $359 million, respectively. Amortization expense for capitalized software for 2009, 2008 and 2007 was $314 million, $290 million and $245 million, respectively.
7. Goodwill and Other Intangible Assets
Changes in the carrying amount of goodwill, by reporting segment, were as follows:
(in millions) | Health Benefits | OptumHealth | Ingenix | Prescription Solutions | Consolidated | ||||||||||||||
Balance at December 31, 2007 | $ | 14,139 | $ | 1,080 | $ | 958 | $ | 677 | $ | 16,854 | |||||||||
Acquisitions | 2,986 | 54 | 74 | 148 | 3,262 | ||||||||||||||
Subsequent payments and adjustments, net | (81 | ) | 18 | 20 | 15 | (28 | ) | ||||||||||||
Balance at December 31, 2008 | 17,044 | 1,152 | 1,052 | 840 | 20,088 | ||||||||||||||
Acquisitions | 161 | 40 | 415 | - | 616 | ||||||||||||||
Subsequent payments and adjustments, net | 61 | (34 | ) | (4 | ) | - | 23 | ||||||||||||
Balance at December 31, 2009 | $ | 17,266 | $ | 1,158 | $ | 1,463 | $ | 840 | $ | 20,727 | |||||||||
74
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The gross carrying value, accumulated amortization and net carrying value of other intangible assets were as follows:
| December 31, 2009 | December 31, 2008 | |||||||||||||||||||
(in millions) | Gross Carrying Value | Accumulated Amortization | Net Carrying Value | Gross Carrying Value | Accumulated Amortization | Net Carrying Value | ||||||||||||||
Customer contracts and membership lists | $ | 2,864 | $ | (796 | ) | $ | 2,068 | $ | 2,620 | $ | (585 | ) | $ | 2,035 | ||||||
Patents, trademarks and technology | 437 | (187 | ) | 250 | 392 | (169 | ) | 223 | ||||||||||||
Other | 118 | (55 | ) | 63 | 120 | (49 | ) | 71 | ||||||||||||
Total | $ | 3,419 | $ | (1,038 | ) | $ | 2,381 | $ | 3,132 | $ | (803 | ) | $ | 2,329 | ||||||
Amortization expense relating to intangible assets for 2009, 2008 and 2007 was $241 million, $252 million and $192 million, respectively.
Estimated full year amortization expense relating to intangible assets for each of the next five years is as follows:
(in millions) | Estimated Amortization Expense | ||
2010 | $ | 255 | |
2011 | 249 | ||
2012 | 247 | ||
2013 | 239 | ||
2014 | 229 | ||
8. Medical Costs and Medical Costs Payable
Medical costs and medical costs payable include estimates of the Company's obligations for medical care services that have been rendered on behalf of insured consumers, but for which claims have either not yet been received or processed, and for liabilities for physician, hospital and other medical cost disputes. The Company develops estimates for medical costs incurred but not reported using an actuarial process that is consistently applied, centrally controlled and automated. The actuarial models consider factors such as time from date of service to claim receipt, claim backlogs, care provider contract rate changes, medical care consumption and other medical cost trends. The Company estimates liabilities for physician, hospital and other medical cost disputes based upon an analysis of potential outcomes, assuming a combination of litigation and settlement strategies. Each period, the Company re-examines previously established medical costs payable estimates based on actual claim submissions and other changes in facts and circumstances. As the medical costs payable estimates recorded in prior periods develop, the Company adjusts the amount of the estimates and includes the changes in estimates in medical costs in the period in which the change is identified.
None of the factors discussed above were individually material to the net favorable medical cost development for the years ended 2009, 2008 and 2007.
75
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The following table shows the components of the change in medical costs payable for the years ended December 31:
(in millions) | 2009 | 2008 | 2007 | |||||||||
Medical costs payable, beginning of period | $ | 8,664 | $ | 8,331 | $ | 8,076 | ||||||
Acquisitions | 252 | 331 | - | |||||||||
Reported medical costs: | ||||||||||||
Current year | 65,599 | 60,589 | 55,855 | |||||||||
Prior years | (310 | ) | (230 | ) | (420 | ) | ||||||
Total reported medical costs | 65,289 | 60,359 | 55,435 | |||||||||
Claim payments: | ||||||||||||
Payments for current year | (57,109 | ) | (52,872 | ) | (48,240 | ) | ||||||
Payments for prior year | (7,734 | ) | (7,485 | ) | (6,940 | ) | ||||||
Total claim payments | (64,843 | ) | (60,357 | ) | (55,180 | ) | ||||||
Medical costs payable, end of period | $ | 9,362 | $ | 8,664 | $ | 8,331 | ||||||
76
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
9. Commercial Paper and Long-Term Debt
Commercial paper and long-term debt consisted of the following:
| December 31, 2009 | December 31, 2008 | |||||||||||||||
(in millions) | Carrying Value (a) | Fair Value (b) | Carrying Value (c) | Fair Value (b) | ||||||||||||
Commercial Paper | $ | - | $ | - | $ | 101 | $ | 101 | ||||||||
$250 million par, 3.8% senior unsecured notes due February 2009 | - | - | 250 | 250 | ||||||||||||
$650 million par, senior unsecured floating-rate notes due March 2009 | - | - | 650 | 644 | ||||||||||||
$450 million par, 4.1% senior unsecured notes due August 2009 | - | - | 455 | 442 | ||||||||||||
$500 million par, senior unsecured floating-rate notes due June 2010 | 500 | 499 | 500 | 450 | ||||||||||||
$250 million par, 5.1% senior unsecured notes due November 2010 | 257 | 259 | 263 | 245 | ||||||||||||
$250 million par, senior unsecured floating-rate notes due February 2011 | 250 | 251 | 250 | 219 | ||||||||||||
$750 million par, 5.3% senior unsecured notes due March 2011 (e) | 781 | 777 | 806 | 705 | ||||||||||||
$450 million par, 5.5% senior unsecured notes due November 2012 (e) | 480 | 481 | 493 | 410 | ||||||||||||
$550 million par, 4.9% senior unsecured notes due February 2013 (e) | 549 | 575 | 549 | 513 | ||||||||||||
$450 million par, 4.9% senior unsecured notes due April 2013 (e) | 464 | 472 | 473 | 419 | ||||||||||||
$250 million par, 4.8% senior unsecured notes due February 2014 (e) | 268 | 256 | 280 | 221 | ||||||||||||
$500 million par, 5.0% senior unsecured notes due August 2014 (e) | 540 | 518 | 567 | 460 | ||||||||||||
$500 million par, 4.9% senior unsecured notes due March 2015 (e) | 544 | 513 | 567 | 429 | ||||||||||||
$750 million par, 5.4% senior unsecured notes due March 2016 (e) | 847 | 772 | 883 | 661 | ||||||||||||
$95 million par, 5.4% senior unsecured notes due November 2016 | 95 | 98 | 95 | 84 | ||||||||||||
$500 million par, 6.0% senior unsecured notes due June 2017 (e) | 587 | 523 | 620 | 450 | ||||||||||||
$250 million par, 6.0% senior unsecured notes due November 2017 (e) | 285 | 258 | 297 | 223 | ||||||||||||
$1,100 million par, 6.0% senior unsecured notes due February 2018 | 1,099 | 1,136 | 1,098 | 1,015 | ||||||||||||
$1,095 million par, zero coupon senior unsecured notes due November 2022 (d) | 558 | 611 | 530 | 522 | ||||||||||||
$850 million par, 5.8% senior unsecured notes due March 2036 | 844 | 762 | 844 | 648 | ||||||||||||
$500 million par, 6.5% senior unsecured notes due June 2037 | 495 | 493 | 495 | 420 | ||||||||||||
$650 million par, 6.6% senior unsecured notes due November 2037 | 645 | 651 | 645 | 548 | ||||||||||||
$1,100 million par, 6.9% senior unsecured notes due February 2038 | 1,085 | 1,138 | 1,083 | 963 | ||||||||||||
Total commercial paper and long-term debt | 11,173 | 11,043 | 12,794 | 11,042 | ||||||||||||
Less commercial paper and current maturities of long-term debt | (2,164 | ) | (2,173 | ) | (1,456 | ) | (1,437 | ) | ||||||||
Long-term debt, less current maturities | $ | 9,009 | $ | 8,870 | $ | 11,338 | $ | 9,605 | ||||||||
| (a) | The carrying value of the debt has been adjusted by the unamortized gain on related interest rate swaps, which terminated in January 2009. |
| (b) | Estimated based on third-party quoted market prices for the same or similar issues. |
| (c) | The carrying value of debt had been adjusted based upon the applicable interest rate swap fair values in accordance with the fair value hedge short-cut method of accounting. |
| (d) | These notes have been classified with the current maturities of long-term debt in the Consolidated Balance Sheet as of December 31, 2009 due to the existence of a put feature. For further discussion, see "Long-Term Debt" below. |
| (e) | A portion of these notes has been classified with the current maturities of long-term debt in the Consolidated Balance Sheet as of December 31, 2009 due to the debt tender offers discussed under "Long-Term Debt" below. |
77
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
Maturities of long-term debt for the years ending December 31 are as follows:
(in millions) | Maturities of Long-Term Debt | ||
2010 | $ | 757 | |
2011 | 985 | ||
2012 | 376 | ||
2013 | 954 | ||
2014 | 605 | ||
Thereafter | 6,089 | ||
$1,095 million par, zero coupon senior unsecured notes due November 2022 | 558 | ||
Debt tender offers completed February 2010 | 849 | ||
Bank Credit Facilities
In November 2008, the Company entered into a $750 million 364-day revolving bank credit facility. The Company terminated this facility on July 31, 2009 in advance of its maturity.
There is currently $2.5 billion available under the Company's five-year revolving bank credit facility, which matures in May 2012. The interest rate is variable based on term and amount and is calculated based on the London Interbank Offered Rate (LIBOR) plus a spread. As of December 31, 2009, the interest rate on this facility, had it been drawn, would have ranged from 0.4% to 0.7%. This facility supports the Company's commercial paper program and is available for general working capital purposes. As of December 31, 2009, the Company had no amounts outstanding under this facility.
Long-Term Debt
In February 2010, the Company completed cash tender offers for $775 million aggregate principal amount of certain of its outstanding notes. The Company believes that this debt repurchase will improve the matching of floating rate assets and liabilities on its balance sheet and reduce its debt service cost. The Company used cash on hand to fund the purchase of the notes.
In February 2008, the Company issued a total of $3.0 billion in senior unsecured debt, which included: $250 million of floating-rate notes due February 2011, $550 million of 4.9% fixed-rate notes due February 2013, $1.1 billion of 6.0% fixed-rate notes due February 2018 and $1.1 billion of 6.9% fixed-rate notes due February 2038. The floating-rate notes are benchmarked to the London Interbank Offered Rate (LIBOR) and had an interest rate of 1.6% as of December 31, 2009.
In November 2007, the Company issued $500 million of zero coupon notes due November 2022. These zero coupon notes are original issue discount notes with an aggregate principal amount due at maturity of $1.1 billion and an accretion yield of 5.3%. These notes have a put feature that allows a note holder to require the Company to repurchase the notes at the accreted value at certain annual dates in the future, beginning on November 15, 2010; therefore, these notes have been classified with the current maturities of long-term debt in the Consolidated Balance Sheet as of December 31, 2009.
In November 2007, the Company issued a total of $1.6 billion in senior unsecured debt, which included: $250 million of 5.1% fixed-rate notes due November 2010, $450 million of 5.5% fixed-rate notes due November 2012, $250 million of 6.0% fixed-rate notes due November 2017 and $650 million of 6.6% fixed-rate notes due November 2037. These notes were issued pursuant to an exemption from registration under Section 4(2) of the
78
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
Securities Act of 1933 (1933 Act). In February 2008, the Company completed an exchange offer in which then-existing noteholders exchanged each series of these notes for a new issue of substantially identical debt securities registered under the 1933 Act.
In June 2007, the Company issued a total of $1.5 billion in senior unsecured debt, which included: $500 million of floating-rate notes due June 2010, $500 million of 6.0% fixed-rate notes due June 2017 and $500 million of 6.5% fixed-rate notes due June 2037. The floating-rate notes are benchmarked to LIBOR and had an interest rate of 0.4% as of December 31, 2009. These notes were issued pursuant to an exemption from registration under Section 4(2) of the 1933 Act. In February 2008, the Company completed an exchange offer in which then-existing noteholders exchanged each series of these notes for a new issue of substantially identical debt securities registered under the 1933 Act.
Debt Covenants
The Company's bank credit facility contains various covenants, the most restrictive of which requires the Company to maintain a debt-to-total-capital ratio, calculated as the sum of commercial paper and debt divided by the sum of commercial paper, debt and shareholders' equity, below 50%. The Company was in compliance with its debt covenants as of December 31, 2009.
Interest Rate Swap Contracts
In January 2009, the Company terminated interest rate swap contracts with $4.9 billion in notional value to lock-in the benefit of low market interest rates. As of the swap contracts' termination date, the cumulative adjustment to the carrying value of the Company's debt was $513 million, which is being amortized over a weighted-average period of 3.5 years as a reduction to interest expense. As of December 31, 2009, the Company had no outstanding interest rate swap contracts. As of December 31, 2008, the fair values of the interest rate swaps were $622 million with $7 million classified in Prepaid Expenses and Other Current Assets and $615 million classified in Other Assets in the Consolidated Balance Sheet.
10. Income Taxes
The components of the provision for income taxes for the years ended December 31 are as follows:
(in millions) | 2009 | 2008 | 2007 | ||||||||
Current Provision: | |||||||||||
Federal | $ | 1,924 | $ | 1,564 | $ | 2,284 | |||||
State and local | 78 | 145 | 166 | ||||||||
Total current provision | 2,002 | 1,709 | 2,450 | ||||||||
Deferred provision | (16 | ) | (62 | ) | 201 | ||||||
Total provision for income taxes | $ | 1,986 | $ | 1,647 | $ | 2,651 | |||||
The reconciliation of the tax provision at the U.S. Federal Statutory Rate to the provision for income taxes for the years ended December 31 is as follows:
(in millions, except percentages) | 2009 | 2008 | 2007 | ||||||||||||||||||
Tax provision at the U.S. federal statutory rate | $ | 2,033 | 35.0 | % | $ | 1,618 | 35.0 | % | $ | 2,557 | 35.0 | % | |||||||||
State income taxes, net of federal benefit | 66 | 1.1 | 106 | 2.2 | 125 | 1.7 | |||||||||||||||
Settlement of state exams, net of federal benefit | (40 | ) | (0.7 | ) | (12 | ) | (0.2 | ) | (5 | ) | - | ||||||||||
Tax-exempt investment income | (70 | ) | (1.2 | ) | (69 | ) | (1.5 | ) | (52 | ) | (0.7 | ) | |||||||||
Other, net | (3 | ) | - | 4 | 0.1 | 26 | 0.3 | ||||||||||||||
Provision for income taxes | $ | 1,986 | 34.2 | % | $ | 1,647 | 35.6 | % | $ | 2,651 | 36.3 | % | |||||||||
79
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
In 2009, the Company released tax reserves related to the favorable resolution of various historical state income tax matters. Along with a change to an insurance premium tax in lieu of an income tax in one of the states in which the Company operates, this decreased the Company's effective income tax rate in 2009.
The components of deferred income tax assets and liabilities as of December 31 are as follows:
(in millions) | 2009 | 2008 | ||||||
Deferred income tax assets: | ||||||||
Share-based compensation | $ | 419 | $ | 413 | ||||
Medical costs payable and other policy liabilities | 218 | 223 | ||||||
Net operating loss carryforwards | 206 | 213 | ||||||
Accrued expenses and allowances | 201 | 93 | ||||||
Long term liabilities | 164 | 354 | ||||||
Unearned revenues | 58 | 56 | ||||||
Unrecognized tax benefits | 55 | 100 | ||||||
Net unrealized losses on investments | - | 15 | ||||||
Other | 190 | 181 | ||||||
Subtotal | 1,511 | 1,648 | ||||||
Less: valuation allowances | (198 | ) | (193 | ) | ||||
Total deferred income tax assets | $ | 1,313 | $ | 1,455 | ||||
Deferred income tax liabilities: | ||||||||
Intangible assets | $ | (890 | ) | $ | (885 | ) | ||
Capitalized software development | (449 | ) | (439 | ) | ||||
Net unrealized gains on investments | (163 | ) | - | |||||
Prepaid expenses | (90 | ) | - | |||||
Depreciation and amortization | (80 | ) | (5 | ) | ||||
Interest rate swaps | - | (230 | ) | |||||
Total deferred income tax liabilities | (1,672 | ) | (1,559 | ) | ||||
Net deferred income tax liabilities | $ | (359 | ) | $ | (104 | ) | ||
Valuation allowances are provided when it is considered more likely than not that deferred tax assets will not be realized. The valuation allowances primarily relate to future tax benefits on certain state net operating loss carryforwards. Federal net operating loss carryforwards of $36 million expire beginning in 2012 through 2026, and state net operating loss carryforwards expire beginning in 2010 through 2028.
A reconciliation of the beginning and ending amount of unrecognized tax benefits as of December 31 is as follows:
(in millions) | 2009 | 2008 | ||||||
Gross unrecognized tax benefits, beginning of period | $ | 340 | $ | 271 | ||||
Gross increases: | ||||||||
Current year tax positions | 10 | 14 | ||||||
Prior year tax positions | 11 | 43 | ||||||
Acquired reserves | - | 94 | ||||||
Gross decreases: | ||||||||
Prior year tax positions | (62 | ) | (29 | ) | ||||
Settlements | (61 | ) | (4 | ) | ||||
Statute of limitations lapses | (18 | ) | (49 | ) | ||||
Gross unrecognized tax benefits, end of period | $ | 220 | $ | 340 | ||||
80
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The favorable resolution of historical state income tax matters resulted in a decrease in the gross unrecognized tax benefits as of December 31, 2009.
The Company classifies interest and penalties associated with uncertain income tax positions as income taxes within its Consolidated Financial Statements. During the year ended December 31, 2009, the Company recognized a net tax benefit of $7 million generated from the reduction in interest accrued from the release of previously accrued tax matters. During the year ended December 31, 2008, the Company recognized $23 million of net interest expense. As of December 31, 2009 and 2008, the Company had $44 million and $65 million, respectively, of accrued interest for uncertain tax positions, which were reported in Accounts Payable and Accrued Liabilities in the Consolidated Balance Sheets. These amounts are not included in the reconciliation above. As of December 31, 2009, the total amount of unrecognized tax benefits that, if recognized, would affect the effective tax rate was $101 million.
The Company currently files income tax returns in the U.S. federal jurisdiction, various states and foreign jurisdictions. The U.S. Internal Revenue Service (IRS) has completed exams on the consolidated income tax returns for fiscal years 2007 and prior. The Company's 2008 and 2009 tax returns are under advance review by the IRS under its Compliance Assurance Program. With the exception of a few states, the Company is no longer subject to income tax examinations prior to 2003 in major state and foreign jurisdictions. The Company does not believe any adjustments that may result from these examinations will be significant.
The Company believes it is reasonably possible that its liability for unrecognized tax benefits will decrease in the next twelve months by $92 million or less as a result of audit settlements and the expiration of statutes of limitations in certain major jurisdictions.
11. Shareholders' Equity
Regulatory Capital and Dividend Restrictions
The Company's regulated subsidiaries are subject to regulations and standards in their respective states of domicile. Most of these regulations and standards conform to those established by the National Association of Insurance Commissioners. These standards, among other things, require these subsidiaries to maintain specified levels of statutory capital, as defined by each state, and restrict the timing and amount of dividends and other distributions that may be paid to their parent companies. Except in the case of extraordinary dividends, these standards generally permit dividends to be paid from statutory unassigned surplus of the regulated subsidiary and are limited based on the regulated subsidiary's level of statutory net income and statutory capital and surplus. These dividends are referred to as "ordinary dividends" and generally can be paid without prior regulatory approval. If the dividend, together with other dividends paid within the preceding twelve months, exceeds a specified statutory limit or is paid from sources other than earned surplus, it is generally considered an "extraordinary dividend" and must receive prior regulatory approval.
In 2009, based on the 2008 statutory net income and statutory capital and surplus levels, the maximum amount of ordinary dividends that could be paid was $3.1 billion. For the year ended December 31, 2009, the Company's regulated subsidiaries paid their parent companies dividends of $4.2 billion, including $2.5 billion of extraordinary dividends. For the year ended December 31, 2008, the Company's regulated subsidiaries paid their parent companies dividends of $4.2 billion, including $1.2 billion of extraordinary dividends. The increase in the proportion of extraordinary dividends to total dividends in 2009 primarily reflects the acceleration of dividend timing, as well as the size of specific dividends beyond ordinary levels. As of December 31, 2009, $2.3 billion of the Company's $24.4 billion of cash and investments was held by non-regulated entities.
The Company's regulated subsidiaries had aggregate statutory capital and surplus of approximately $10 billion as of December 31, 2009, which exceeds aggregate minimum regulatory requirements.
81
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
Share Repurchase Program
Under its Board of Directors' authorization, the Company maintains a share repurchase program (Repurchase Program). The objectives of the Repurchase Program are to optimize the Company's capital structure and cost of capital, thereby improving returns to shareholders, as well as to offset the dilutive impact of share-based awards. Repurchases may be made from time to time at prevailing prices in the open market. During 2009, the Company repurchased 74.3 million shares at an average price of approximately $24 per share and an aggregate cost of $1.8 billion. As of December 31, 2009, the Company had Board of Directors' authorization to purchase up to an additional 28.7 million shares of its common stock. In February 2010, the Board renewed and increased the Company's share repurchase program, and authorized the Company to repurchase up to 120 million shares of its common stock.
12. Share-Based Compensation and Other Employee Benefit Plans
The Company's 2002 Stock Incentive Plan (Plan), as amended and restated May 15, 2002, is intended to attract and retain employees and non-employee directors, offer them incentives to put forth maximum efforts for the success of the Company's business and afford them an opportunity to acquire a proprietary interest in the Company. The Plan allows the Company to grant stock options, stock appreciation rights, restricted stock, restricted stock units, performance awards or other stock-based awards to eligible employees and non-employee directors. The Plan incorporates the following prior plans: 1991 Stock and Incentive Plan, 1998 Broad-Based Stock Incentive Plan and Non-employee Director Stock Option Plan. All outstanding stock options, restricted stock and other awards issued under the prior plans shall remain subject to the terms and conditions of these plans under which they were issued.
As of December 31, 2009, the Company had 63.5 million shares available for future grants of share-based awards under its share-based compensation plan, including, but not limited to, incentive or non-qualified stock options, stock-settled stock appreciation rights (SARs), and up to 15.3 million of awards in restricted stock and restricted stock units (collectively, restricted shares). The Company's outstanding share-based awards consist mainly of non-qualified stock options, SARs and restricted shares.
Stock Options and SARs
Stock options and SARs generally vest ratably over four to six years and may be exercised up to 10 years from the date of grant. Stock option and SAR activity for the year ended December 31, 2009 is summarized in the table below:
| Shares | Weighted- Average Exercise Price | Weighted-Average Remaining Contractual Life | Aggregate Intrinsic Value | ||||||||
| (in thousands) | (in years) | (in millions) | |||||||||
Outstanding, beginning of period | 150,752 | $ | 36 | ||||||||
Granted | 15,026 | 30 | |||||||||
Exercised | (19,421 | ) | 13 | ||||||||
Forfeited | (22,211 | ) | 34 | ||||||||
Outstanding, end of period | 124,146 | $ | 39 | 5.5 | $ | 304 | |||||
Exercisable, end of period | 87,664 | $ | 39 | 4.4 | $ | 287 | |||||
Vested and expected to vest at end of period | 118,962 | $ | 39 | 5.3 | $ | 302 | |||||
82
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
To determine compensation expense related to the Company's stock options and SARs, the fair value of each award is estimated on the date of grant using an option-pricing model. For purposes of estimating the fair value of the Company's employee stock option and SAR grants, the Company uses a binomial model. The principal assumptions the Company used in applying the option-pricing models were as follows:
| 2009 | 2008 | 2007 | ||||
Risk free interest rate | 1.7% - 2.4% | 2.2% - 3.4% | 3.8% - 5.2% | |||
Expected volatility | 41.3% - 46.8% | 29.5% | 24.2% | |||
Expected dividend yield | 0.1% | 0.1% | 0.1% | |||
Forfeiture rate | 5.0% | 5.0% | 5.0% | |||
Expected life in years | 4.4 - 5.1 | 4.3 | 4.1 |
Risk-free interest rates are based on U.S. Treasury yields in effect at the time of grant. Expected volatilities are based on the historical volatility of the Company's common stock and the implied volatility from exchange-traded options on the Company's common stock. Beginning in 2009, the Company changed the weighting of historical and implied volatilities used in the calculation of expected volatility to 90% and 10%, respectively. Before the change, the Company had weighted historical and implied volatility equally. Due to the significant economic turbulence and resulting instability of the exchange-traded options throughout 2008, the Company concluded that they were no longer as representative of the fair value of its common stock over the expected life of its options and SARs. The change had no impact on the Company's reported Net Earnings nor Earnings per Share. The Company uses historical data to estimate option and SAR exercises and forfeitures within the valuation model. The expected lives of options and SARs granted represents the period of time that the awards granted are expected to be outstanding based on historical exercise patterns.
The weighted-average grant date fair value of stock options and SARs granted for 2009, 2008 and 2007 was approximately $10 per share, $9 per share and $14 per share. The total intrinsic value of stock options and SARs exercised during 2009, 2008 and 2007 was $282 million, $244 million and $1.1 billion, respectively.
Restricted Shares
Restricted shares generally vest ratably over two to five years. Compensation expense related to restricted shares is based on the share price on date of grant. Restricted share activity for the year ended December 31, 2009 is summarized in the table below:
(shares in thousands) | Shares | Weighted- Average Grant Date Fair Value | ||||
Nonvested, Beginning of Period | 6,282 | $ | 36 | |||
Granted | 6,587 | 29 | ||||
Vested | (1,655 | ) | 29 | |||
Forfeited | (594 | ) | 34 | |||
Nonvested, End of Period | 10,620 | $ | 33 | |||
The weighted-average grant date fair value of restricted shares granted during 2009, 2008 and 2007 was approximately $29 per share, $34 per share and $51 per share, respectively. The total fair value of restricted shares vested during 2009, 2008 and 2007 was $47 million, $17 million and $35 million, respectively.
83
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
Employee Stock Purchase Plan
The Company's Employee Stock Purchase Plan (ESPP) is intended to enhance employee commitment to the goals of the Company, by providing a means of achieving stock ownership at advantageous terms to eligible employees of the Company. Eligible employees are allowed to purchase the Company's stock at a discounted price, which is 85% of the lower market price of the Company's common stock at the beginning or at the end of the six-month purchase period. During 2009, 2008 and 2007, 3.7 million shares, 2.9 million shares and 1.9 million shares of common stock, respectively, were purchased under the ESPP. The compensation expense is included in the compensation expense amounts recognized and discussed below. As of December 31, 2009, there were 9.3 million shares of common stock available for issuance under the ESPP.
Share-Based Compensation Recognition
The Company recognizes compensation expense for share-based awards, including stock options, SARs and restricted shares, on a straight-line basis over the related service period (generally the vesting period) of the award, or to an employee's eligible retirement date under the award agreement, if earlier. Beginning with share-based awards granted in 2009, the Company's equity award program includes a retirement provision that treats all employees who are age 55 or older with at least ten years of recognized employment with the Company as retirement-eligible. For 2009, 2008 and 2007, the Company recognized compensation expense related to its share-based compensation plans of $334 million ($220 million net of tax effects), $305 million ($202 million net of tax effects) and $505 million ($325 million net of tax effects), respectively. Share-based compensation expense is recognized in Operating Costs in the Company's Consolidated Statements of Operations. As of December 31, 2009, there was $490 million of total unrecognized compensation cost related to share awards that is expected to be recognized over a weighted-average period of 1.4 years. For 2009, 2008 and 2007, the income tax benefit realized from share-based award exercises was $94 million, $106 million and $399 million, respectively.
Included in the share-based compensation expense for the year ended December 31, 2007 is $176 million ($112 million net of tax benefit) of expenses recorded in the first quarter of 2007 related to application of deferred compensation rules under Section 409A of the Internal Revenue Code (Section 409A) to the Company's historical stock option practices. As part of its review of the Company's historical stock option practices, the Company determined that certain stock options granted to individuals who were nonexecutive officer employees at the time of grant were granted with an exercise price that was lower than the closing price of the Company's common stock on the applicable accounting measurement date, subjecting these individuals to additional tax under Section 409A. The Company elected to pay these individuals for the additional tax costs relating to such stock options exercised in 2006 and early 2007. For any outstanding stock options subject to additional tax under Section 409A that were granted to nonexecutive officer employees, the Company increased the exercise price and committed to make cash payments to these optionholders for their vested options based on the difference between the original stock option price and the revised increased stock option price. Payments of $142 million were made from January 2008 through January 2010 for options vested through December 31, 2009. If the modified stock options are subsequently exercised, the Company will recover these cash payments at that time from exercise proceeds at the revised increased stock option exercise prices.
The $176 million Section 409A charge includes $87 million of expense ($55 million net of tax benefit) for the payment of certain optionholders' tax obligations for stock options exercised in 2006 and early 2007 and $89 million of expense ($57 million net of tax benefit) for the modification related to increasing the exercise price of unexercised stock options granted to nonexecutive officer employees and the related cash payments. These amounts have been recorded in the corporate segment.
84
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
As further discussed in Note 11 of Notes to the Consolidated Financial Statements, the Company maintains a share repurchase program. The objectives of the share repurchase program are to optimize the Company's capital structure, cost of capital and return to shareholders, as well as to offset the dilutive impact of shares issued for share-based award exercises.
Other Employee Benefit Plans
The Company also offers a 401(k) plan for all employees. Compensation expense related to this plan was not significant for the years 2009, 2008 and 2007.
The Company has provided Supplemental Executive Retirement Plan (SERP) benefits, which are non-qualified defined benefit plans, for its CEO, as well as for certain nonexecutive officers under plans that were assumed in acquisitions. No additional amounts are accruing to the SERP for the Company's CEO. The SERPs are non-contributory, unfunded and provide benefits based on years of service and compensation during employment. The total SERP liability as of December 31, 2009 was $20 million, which was recorded in Other Liabilities in the Consolidated Balance Sheets. The total SERP liability as of December 31, 2008 was $159 million, of which $51 million was recorded in Accounts Payable and Accrued Liabilities and $108 million was recorded in Other Liabilities in the Consolidated Balance Sheets. In 2009, a SERP accrual of $91 million relating to the Company's former CEO was reversed as a result of the resolution of the SEC settlement pertaining to the stock option matter. See Note 14 of Notes to the Consolidated Financial Statements for further discussion of stock option matters.
In addition, the Company maintains non-qualified, unfunded deferred compensation plans, which allow certain members of senior management and executives to defer portions of their salary or bonus and receive certain Company contributions on such deferrals, subject to plan limitations. The deferrals are recorded within Long-Term Investments with an approximately equal amount in Other Liabilities in the Consolidated Balance Sheets. The total deferrals are distributable based upon termination of employment or other periods, as elected under each plan and were $216 million and $182 million as of December 31, 2009 and 2008, respectively.
13. AARP
The Company provides health insurance products and services to members of AARP under a Supplemental Health Insurance Program (the Program), and separate Medicare Advantage and Medicare Part D arrangements. The products and services under the Program include supplemental Medicare benefits (AARP Medicare Supplement Insurance), hospital indemnity insurance, including insurance for individuals between 50 to 64 years of age, and other related products.
In October 2007, the Company entered into four agreements with AARP, effective January 1, 2008, that amended its existing AARP arrangements. These agreements extended the Company's arrangements with AARP on the Program to December 31, 2017, extended the Company's arrangement with AARP on the Medicare Part D business to December 31, 2014, and gave the Company an exclusive right to use the AARP brand on the Company's Medicare Advantage offerings until December 31, 2014, subject to certain limited exclusions.
Under the Program, the Company is compensated for transaction processing and other services, as well as for assuming underwriting risk. The Company is also engaged in product development activities to complement the insurance offerings. Premium revenues from the Company's portion of the Program for 2009, 2008 and 2007 were $6.0 billion, $5.7 billion and $5.3 billion, respectively.
The Company's agreement with AARP on the Program provides for the maintenance of the Rate Stabilization Fund (RSF) that is held by the Company on behalf of policyholders. Underwriting gains or losses related to the
85
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
AARP Medicare Supplement Insurance business are directly recorded as an increase or decrease to the RSF. The primary components of the underwriting results are premium revenue, medical costs, investment income, administrative expenses, member service expenses, marketing expenses and premium taxes. Underwriting gains and losses are recorded as an increase or decrease to the RSF and accrue to the overall benefit of the AARP policyholders, unless cumulative net losses were to exceed the balance in the RSF. To the extent underwriting losses exceed the balance in the RSF, losses would be borne by the Company. Deficits may be recovered by underwriting gains in future periods of the contract. To date, the Company has not been required to fund any underwriting deficits. The RSF balance is reported in Other Policy Liabilities in the Consolidated Balance Sheets and changes in the RSF are reported in Medical Costs in the Consolidated Statement of Operations. In January 2008, $127 million in cash was transferred out of the RSF to an external insurance entity that offers an AARP branded age 50 to 64 comprehensive insurance product. The Company believes the RSF balance as of December 31, 2009 is sufficient to cover potential future underwriting and other risks and liabilities associated with the contract.
The effects of changes in balance sheet amounts associated with the Program also accrue to the overall benefit of the AARP policyholders through the RSF balance. Accordingly, the Company excludes the effect of such changes in its Consolidated Statements of Cash Flows.
Under the Company's agreement with AARP, the Company separately manages the assets that support the Program. These assets are held at fair value in the Consolidated Balance Sheets as Assets Under Management. These assets are invested at the Company's discretion, within investment guidelines approved by the Program and are used to pay costs associated with the Program. The Company does not guarantee any rates of investment return on these investments and upon any transfer of the Program to another entity, the Company would transfer cash in an amount equal to the fair value of these investments at the date of transfer. Interest earnings and realized investment gains and losses on these assets accrue to the overall benefit of the AARP policyholders through the RSF and, thus, are not included in the Company's earnings. Interest income and realized gains and losses related to assets under management are recorded as an increase to the AARP RSF and were $99 million, $82 million and $108 million in 2009, 2008 and 2007, respectively.
The Company elected to measure the entirety of the AARP Assets Under Management at fair value, pursuant to the fair value option.
The following AARP Program-related assets and liabilities were included in the Company's Consolidated Balance Sheets:
(in millions) | December 31, 2009 | December 31, 2008 | ||||
Accounts receivable | $ | 509 | $ | 482 | ||
Assets under management | 2,383 | 2,199 | ||||
Other assets | - | 7 | ||||
Medical costs payable | 1,182 | 1,160 | ||||
Accounts payable and accrued liabilities | 40 | 52 | ||||
Other policy liabilities | 1,145 | 1,047 | ||||
Future policy benefits | 482 | 429 | ||||
Other liabilities | 43 | - | ||||
86
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The fair value of cash, cash equivalents and investments associated with the Program, reflected as Assets Under Management, and the fair value of Other Assets and Other Liabilities were classified in accordance with the fair value hierarchy as discussed in Note 5 of Notes to the Consolidated Financial Statements and were as follows:
(in millions) | Quoted Prices in Active Markets (Level 1) | Other Observable Inputs (Level 2) | Unobservable Inputs (Level 3) | Total Fair Value | ||||||||
December 31, 2009 | ||||||||||||
Cash and cash equivalents | $ | 269 | $ | - | $ | - | $ | 269 | ||||
Debt securities: | ||||||||||||
U.S. government and agency obligations | 358 | 298 | - | 656 | ||||||||
State and municipal obligations | - | 9 | - | 9 | ||||||||
Corporate obligations | - | 955 | - | 955 | ||||||||
U.S. agency mortgage-backed securities | - | 343 | - | 343 | ||||||||
Non-U.S. agency mortgage-backed securities | - | 149 | - | 149 | ||||||||
Total debt securities | 358 | 1,754 | - | 2,112 | ||||||||
Equity securities - available-for-sale | - | 2 | - | 2 | ||||||||
Total cash, cash equivalents and investments at fair value | $ | 627 | $ | 1,756 | $ | - | $ | 2,383 | ||||
Other liabilities | $ | - | $ | - | $ | 43 | $ | 43 | ||||
Total liabilities at fair value | $ | - | $ | - | $ | 43 | $ | 43 | ||||
December 31, 2008 | ||||||||||||
Cash and cash equivalents | $ | 240 | $ | 18 | $ | - | $ | 258 | ||||
Debt securities: | ||||||||||||
U.S. government and agency obligations | 291 | 293 | - | 584 | ||||||||
State and municipal obligations | - | 6 | - | 6 | ||||||||
Corporate obligations | - | 786 | - | 786 | ||||||||
U.S. agency mortgage-backed securities | - | 421 | - | 421 | ||||||||
Non-U.S. agency mortgage-backed securities | - | 142 | - | 142 | ||||||||
Total debt securities | 291 | 1,648 | - | 1,939 | ||||||||
Equity securities - available-for-sale | - | 2 | - | 2 | ||||||||
Total cash, cash equivalents and investments at fair value | 531 | 1,668 | - | 2,199 | ||||||||
Other assets | - | - | 7 | 7 | ||||||||
Total assets at fair value | $ | 531 | $ | 1,668 | $ | 7 | $ | 2,206 | ||||
14. Commitments and Contingencies
The Company leases facilities, computer hardware and other equipment under long-term operating leases that are noncancelable and expire on various dates through 2028. Rent expense under all operating leases for 2009, 2008 and 2007 was $303 million, $264 million and $223 million, respectively.
87
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
As of December 31, 2009, future minimum annual lease payments, net of sublease income, under all noncancelable operating leases were as follows:
(in millions) | Future Minimum Lease Payments | ||
2010 | $ | 255 | |
2011 | 221 | ||
2012 | 199 | ||
2013 | 152 | ||
2014 | 120 | ||
Thereafter | 644 | ||
The Company contracts on an administrative services only (ASO) basis with customers who fund their own claims. The Company charges these customers administrative fees based on the expected cost of administering their self-funded programs. In some cases, the Company provides performance guarantees related to its administrative function. If these standards are not met, the Company may be financially at risk up to a stated percentage of the contracted fee or a stated dollar amount. Amounts accrued for performance guarantees were not material as of December 31, 2009 and 2008.
As of December 31, 2009, the Company has outstanding, undrawn letters of credit with financial institutions of $62 million and surety bonds outstanding with insurance companies of $247 million, primarily to bond contractual performance.
Legal Matters
Because of the nature of its businesses, the Company is frequently made party to a variety of legal actions and regulatory inquiries related to, among other things, the design and management of its service offerings. The Company records liabilities for its estimates of probable costs resulting from these matters where appropriate. These matters include, but are not limited to, claims relating to health care benefits coverage, medical malpractice actions, contract disputes and claims related to certain business practices.
Litigation Matters
MDL Litigation. Beginning in 1999, a series of class action lawsuits were filed against the Company by health care providers alleging various claims relating to the Company's reimbursement practices, including alleged violations of the Racketeer Influenced Corrupt Organization Act (RICO) and state prompt payment laws and breach of contract claims. Many of these lawsuits were consolidated in a multi-district litigation in the United States District Court for the Southern District Court of Florida (MDL). In the lead MDL lawsuit, the court certified a class of health care providers for certain of the RICO claims. In 2006, the trial court dismissed all of the claims against the Company in the lead MDL lawsuit, and the Eleventh Circuit Court of Appeals later affirmed that dismissal, leaving eleven related lawsuits that had been stayed during the litigation of the lead MDL lawsuit. In August 2008, the trial court, applying its rulings in the lead MDL lawsuit, dismissed seven of the 11 related lawsuits, and all but one claim in an eighth lawsuit. The plaintiffs have appealed these dismissals to the Eleventh Circuit. The trial court ordered the final claim in the eighth lawsuit to arbitration. In December 2008, at the plaintiffs' request, the trial court dismissed without prejudice one of the three remaining lawsuits. The court also denied the plaintiffs' request to remand the remaining two lawsuits to state court and a federal magistrate judge recommended dismissal of those suits. On April 16, 2009, the plaintiffs in these last two suits filed amended class action complaints alleging breach of contract. In addition, the Company is party to a number of arbitrations in various jurisdictions involving similar claims. The Company is vigorously defending against the remaining claims in these cases.
88
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
AMA Litigation. On March 15, 2000, a group of plaintiffs including the American Medical Association (AMA) filed a lawsuit against the Company in state court in New York, which was removed to federal court. The complaint and subsequent amended complaints asserted antitrust claims and claims based on the Employee Retirement Income Security Act of 1974, as amended (ERISA), as well as breach of contract and the implied covenant of good faith and fair dealing, deceptive acts and practices, and trade libel in connection with the calculation of reasonable and customary reimbursement rates for non-network health care providers by the Company's affiliates. On January 14, 2009, after almost nine years of litigation and many rulings from the court on various motions, the parties announced an agreement to settle the lawsuit, along with a similar case filed in 2008 in federal court in New Jersey. Under the terms of the proposed settlement, the Company and its affiliated entities will be released from claims relating to their out-of-network reimbursement policies from March 15, 1994 through the date of final court approval of the settlement. The Company will pay a total of $350 million to fund the settlement for health plan members and out-of-network providers in connection with out-of-network procedures performed since March 15, 1994. The agreement contains no admission of wrongdoing. The proposed settlement is subject to final court approval. In addition, the Company has the right to terminate the settlement if a certain number of class members elect to opt-out of the settlement. A splinter group of plaintiffs' counsel is challenging the proposed settlement. The court granted preliminary approval of the proposed settlement over the objections of certain plaintiffs' counsel on December 1, 2009, and a final approval hearing following notice to members of the class is scheduled for July 2010. Other lawsuits in various jurisdictions relating to the calculation of reasonable and customary reimbursement rates for non-network health care providers remain pending against a number of health insurers, including the Company.
NYAG Investigation. On February 13, 2008, the Office of the Attorney General of the State of New York (NYAG) announced that it was conducting an industry-wide investigation into out-of-network provider reimbursement practices of health insurers, including the Company, and served the Company with a notice of intent to initiate litigation. On January 13, 2009, the Company announced it had reached an agreement with the NYAG regarding the investigation. Under the terms of the agreement, the Company agreed to pay $50 million to fund a not-for-profit entity to develop and own a new, independent database product to replace the Prevailing Health Charges System (PHCS) and Medical Data Research (MDR) database products owned by Ingenix, Inc. Both products are used by a number of health plans and employers as tools that help determine the amount to reimburse members who receive physician services outside their managed care networks. When the new database product is ready, the Company will cease using the PHCS and MDR databases and will use the new database for a period of at least five years in connection with out-of-network reimbursement in those benefit plans that employ a reasonable and customary standard for out-of-network reimbursements. On October 2, 2009, the Company paid the $50 million required under the settlement agreement into an account designated by the NYAG. Following the announcement of the NYAG settlement, the Company received inquiries from a number of state and federal regulators, including the U.S. Senate Commerce Committee, regarding out-of-network reimbursement practices of health insurers.
California Claims Processing Matter. As previously disclosed, in 2007, the California Department of Insurance (CDI) examined the Company's PacifiCare health insurance plan in California. The examination findings related to the timeliness and accuracy of claims processing, interest payments, provider contract implementation, provider dispute resolution, and other related matters. On January 25, 2008, the CDI issued an Order to Show Cause to PacifiCare Life and Health Insurance Company, a subsidiary of the Company, alleging violations of certain insurance statutes and regulations in connection with the CDI's examination findings. On June 3, 2009, the Company filed a Notice of Defense to the Order to Show Cause denying all material allegations and asserting certain defenses. The matter is now the subject of an administrative hearing before a California administrative law judge.
Historical Stock Option Practices. In 2006, a consolidated shareholder derivative action, captioned In re UnitedHealth Group Incorporated Shareholder Derivative Litigation was filed against certain of the Company's
89
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
current and former officers and directors in the United States District Court for the District of Minnesota. The
consolidated amended complaint was brought on behalf of the Company by several pension funds and other shareholders and named certain of the Company's current and former officers and directors as defendants, as well as the Company as a nominal defendant. The consolidated amended complaint generally alleged that the defendants breached their fiduciary duties to the Company, were unjustly enriched, and violated the securities laws in connection with the Company's historical stock option practices. On June 26, 2006, the Company's Board of Directors created a Special Litigation Committee under Minnesota Statute 302A.241, consisting of two former Minnesota Supreme Court Justices, with the power to investigate the claims raised in the derivative actions and shareholder demands and determine whether the Company's rights and remedies should be pursued.
A consolidated derivative action, captioned In re UnitedHealth Group Incorporated Derivative Litigation , was also filed in Hennepin County District Court, State of Minnesota. The action was brought by two individual shareholders and named certain of the Company's current and former officers and directors as defendants, as well as the Company as a nominal defendant.
On December 6, 2007, the Special Litigation Committee concluded its review of claims relating to the Company's historical stock option practices and published a report. The Special Litigation Committee reached settlement agreements on behalf of the Company with its former Chairman and Chief Executive Officer William W. McGuire, M.D., former General Counsel David J. Lubben, and former director William G. Spears. In addition, the Special Litigation Committee concluded that all claims against all named defendants in the derivative actions, including current and former Company officers and directors, should be dismissed. Each settlement agreement is conditioned upon dismissal of claims in the derivative actions and resolution of any appeals. Following notice to shareholders, the federal court granted the parties' motion for final approval of the proposed settlements on July 1, 2009, and entered final judgment dismissing the federal case with prejudice on July 2, 2009. The state court granted the parties' motion for final approval of the proposed settlements and dismissed the state case with prejudice on May 14, 2009, and entered final judgment on July 17, 2009. The federal and state courts also awarded plaintiffs' counsel fees and expenses of $30 million and $6 million, respectively, which have been paid by the Company. A shareholder has filed an appeal with the U.S. Court of Appeals for the Eighth Circuit challenging only the federal plaintiffs' counsel's fee award. Federal plaintiffs' counsel is contesting the appeal.
As previously disclosed, the Company also received inquiries from a number of federal and state regulators from 2006 through 2008 regarding its historical stock option practices. Many of those inquiries have been closed, resolved or inactive since 2008.
The Company may be subject to additional litigation or other proceedings or actions arising out of the Company's historical stock option practices and the related restatement of its historical Consolidated Financial Statements. Litigation and any potential regulatory proceeding or action may be time consuming, expensive and distracting from the conduct of the Company's business. The adverse resolution of any specific lawsuit or any potential regulatory proceeding or action could have a material adverse effect on the Company's business, financial condition and results of operations.
Government Regulation
The Company's business is regulated at federal, state, local and international levels. The laws and rules governing the Company's business and interpretations of those laws and rules are subject to frequent change. Broad latitude is given to the agencies administering those regulations. State legislatures and Congress continue to focus on health care issues as the subject of proposed legislation. In connection with these activities, the Company periodically receives inquiries and requests for information from state or federal legislative bodies. For instance, during the third and fourth quarters of 2009, the Company received requests for information and
90
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
testimony from Congressional committees in connection with health care reform legislative proposals. The Company is cooperating with these requests. Existing or future laws and rules could force us to change how the Company does business, restrict revenue and enrollment growth, increase the Company's health care and administrative costs and capital requirements, and increase the Company's liability in federal and state courts for coverage determinations, contract interpretation and other actions. Further, the Company must obtain and maintain regulatory approvals to market and sell many of its products.
The Company has been and is currently involved in various governmental investigations, audits and reviews. These include routine, regular and special investigations, audits and reviews by CMS, state insurance and health and welfare departments, state attorneys general, the Office of the Inspector General, the Office of Personnel Management, the Office of Civil Rights, U.S. Congressional committees, the U.S. Department of Justice, U.S. Attorneys, the SEC, the IRS, the U.S. Department of Labor and other governmental authorities.
Examples of audits include a review by the U.S. Department of Labor of the Company's administration of applicable customer employee benefit plans with respect to ERISA compliance and audits of the Company's Medicare health plans to validate the coding practices of and supporting documentation maintained by its care providers.
Such government actions can result in assessment of damages, civil or criminal fines or penalties, or other sanctions, including loss of licensure or exclusion from participation in government programs and could have a material adverse effect on the Company's financial results. The coding audits may result in prospective and retrospective adjustments to payments made to health plans pursuant to CMS Medicare contracts.
15. Segment Financial Information
Factors used in determining the Company's reporting segments include the nature of operating activities, economic characteristics, existence of separate senior management teams and the type of information presented to the Company's chief operating decision-maker to evaluate its results of operations.
The Company's accounting policies for reporting segment operations are the same as those described in the Summary of Significant Accounting Policies (see Note 2 of Notes to the Consolidated Financial Statements). Transactions between reporting segments principally consist of sales of pharmacy benefit products and services to Health Benefits customers by Prescription Solutions, certain product offerings sold to Health Benefits customers by OptumHealth, and medical benefits cost, quality and utilization data and predictive modeling sold to Health Benefits by Ingenix. These transactions are recorded at management's estimate of fair value. Intersegment transactions are eliminated in consolidation. Assets and liabilities that are jointly used are assigned to each reporting segment using estimates of pro-rata usage. Cash and investments are assigned such that each reporting segment has at least minimum specified levels of regulatory capital or working capital for non-regulated businesses.
Substantially all of the Company's assets are held and operations are conducted in the United States. In accordance with accounting principles generally accepted in the United States, reporting segments with similar economic characteristics may be combined. The financial results of UnitedHealthcare, Ovations and AmeriChoice have been aggregated in the Health Benefits segment column in the following tables because these businesses have similar economic characteristics and have similar products and services, types of customers, distribution methods and operational processes, and operate in a similar regulatory environment. These businesses also share significant common assets, including the Company's contracted networks of physicians, health care professionals, hospitals and other facilities, information technology infrastructure and other resources.
As a percentage of the Company's total consolidated revenues, premium revenues from CMS were 27% for the year ended December 31, 2009, and 25% for the years ended December 31, 2008 and 2007 most of which were generated by Ovations and included in the Health Benefits segment.
91
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
The following table presents reporting segment financial information as of and for the years ended December 31:
(in millions) | Health Benefits | OptumHealth | Ingenix | Prescription Solutions | Corporate and Intersegment Eliminations | Consolidated | ||||||||||||||
2009 | ||||||||||||||||||||
Revenues - External Customers: | ||||||||||||||||||||
Premiums | $ | 76,882 | $ | 2,433 | $ | - | $ | - | $ | - | $ | 79,315 | ||||||||
Services | 3,937 | 277 | 1,042 | 50 | - | 5,306 | ||||||||||||||
Products | - | - | 90 | 1,835 | - | 1,925 | ||||||||||||||
Total revenues - external customers | 80,819 | 2,710 | 1,132 | 1,885 | - | 86,546 | ||||||||||||||
Total revenues - intersegment | - | 2,753 | 691 | 12,562 | (16,006 | ) | - | |||||||||||||
Investment and other income | 522 | 65 | - | 5 | - | 592 | ||||||||||||||
Total revenues | $ | 81,341 | $ | 5,528 | $ | 1,823 | $ | 14,452 | $ | (16,006 | ) | $ | 87,138 | |||||||
Earnings from operations | $ | 4,788 | $ | 636 | $ | 246 | $ | 689 | $ | - | $ | 6,359 | ||||||||
Interest expense | - | - | - | - | (551 | ) | (551 | ) | ||||||||||||
Earnings before income taxes | $ | 4,788 | $ | 636 | $ | 246 | $ | 689 | $ | (551 | ) | $ | 5,808 | |||||||
Total assets | $ | 49,068 | $ | 4,395 | $ | 2,415 | $ | 3,061 | $ | 106 | $ | 59,045 | ||||||||
Purchases of property, equipment and capitalized software | $ | 452 | $ | 78 | $ | 142 | $ | 67 | $ | - | $ | 739 | ||||||||
Depreciation and Amortization | $ | 668 | $ | 116 | $ | 129 | $ | 78 | $ | - | $ | 991 | ||||||||
2008 | ||||||||||||||||||||
Revenues - External Customers: | ||||||||||||||||||||
Premiums | $ | 71,298 | $ | 2,310 | $ | - | $ | - | $ | - | $ | 73,608 | ||||||||
Services | 3,871 | 311 | 925 | 45 | - | 5,152 | ||||||||||||||
Products | - | - | 95 | 1,560 | - | 1,655 | ||||||||||||||
Total Revenues - External Customers | 75,169 | 2,621 | 1,020 | 1,605 | - | 80,415 | ||||||||||||||
Total Revenues - Intersegment | - | 2,529 | 532 | 10,960 | (14,021 | ) | - | |||||||||||||
Investment and Other Income | 688 | 75 | - | 8 | - | 771 | ||||||||||||||
Total Revenues | $ | 75,857 | $ | 5,225 | $ | 1,552 | $ | 12,573 | $ | (14,021 | ) | $ | 81,186 | |||||||
Earnings from Operations | $ | 5,068 | $ | 718 | $ | 229 | $ | 363 | $ | (1,115 | ) | $ | 5,263 | |||||||
Interest expense | - | - | - | - | (639 | ) | (639 | ) | ||||||||||||
Earnings before income taxes | $ | 5,068 | $ | 718 | $ | 229 | $ | 363 | $ | (1,754 | ) | $ | 4,624 | |||||||
Total Assets | $ | 46,459 | $ | 4,195 | $ | 1,755 | $ | 2,603 | $ | 803 | $ | 55,815 | ||||||||
Purchases of Property, Equipment and Capitalized Software | $ | 522 | $ | 100 | $ | 112 | $ | 57 | $ | - | $ | 791 | ||||||||
Depreciation and Amortization | $ | 691 | $ | 120 | $ | 105 | $ | 65 | $ | - | $ | 981 | ||||||||
2007 | ||||||||||||||||||||
Revenues - External Customers: | ||||||||||||||||||||
Premiums | $ | 66,625 | $ | 2,156 | $ | - | $ | - | $ | - | $ | 68,781 | ||||||||
Services | 3,530 | 292 | 767 | 19 | - | 4,608 | ||||||||||||||
Products | - | - | 100 | 798 | - | 898 | ||||||||||||||
Total Revenues - External Customers | 70,155 | 2,448 | 867 | 817 | - | 74,287 | ||||||||||||||
Total Revenues - Intersegment | - | 2,385 | 437 | 12,420 | (15,242 | ) | - | |||||||||||||
Investment and Other Income | 1,044 | 88 | - | 12 | - | 1,144 | ||||||||||||||
Total Revenues | $ | 71,199 | $ | 4,921 | $ | 1,304 | $ | 13,249 | $ | (15,242 | ) | $ | 75,431 | |||||||
Earnings from Operations | $ | 6,595 | $ | 895 | $ | 266 | $ | 269 | $ | (176 | ) | $ | 7,849 | |||||||
Interest expense | - | - | - | - | (544 | ) | (544 | ) | ||||||||||||
Earnings before income taxes | $ | 6,595 | $ | 895 | $ | 266 | $ | 269 | $ | (720 | ) | $ | 7,305 | |||||||
Total Assets | $ | 43,343 | $ | 3,714 | $ | 1,596 | $ | 2,420 | $ | (174 | ) | $ | 50,899 | |||||||
Purchases of Property, Equipment and Capitalized Software | $ | 623 | $ | 108 | $ | 121 | $ | 19 | $ | - | $ | 871 | ||||||||
Depreciation and Amortization | $ | 559 | $ | 111 | $ | 81 | $ | 45 | $ | - | $ | 796 | ||||||||
92
UNITEDHEALTH GROUP
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS-(Continued)
16. Quarterly Financial Data (Unaudited)
Selected quarterly financial information for all quarters of 2009 and 2008 is as follows:
| For the Quarter Ended | ||||||||||||
(in millions, except per share data) | March 31 | June 30 | September 30 | December 31 | ||||||||
2009 | ||||||||||||
Revenues | $ | 22,004 | $ | 21,655 | $ | 21,695 | $ | 21,784 | ||||
Operating costs | 20,336 | 20,215 | 20,019 | 20,209 | ||||||||
Earnings from operations | 1,668 | 1,440 | 1,676 | 1,575 | ||||||||
Net earnings | 984 | 859 | 1,035 | 944 | ||||||||
Basic net earnings per common share | 0.82 | 0.73 | 0.90 | 0.82 | ||||||||
Diluted net earnings per common share | 0.81 | 0.73 | 0.89 | 0.81 | ||||||||
2008 | ||||||||||||
Revenues | $ | 20,304 | $ | 20,272 | $ | 20,156 | $ | 20,454 | ||||
Operating costs | 18,591 | 19,599 | 18,558 | 19,175 | ||||||||
Earnings from operations | 1,713 | 673 | 1,598 | 1,279 | ||||||||
Net earnings | 994 | 337 | 920 | 726 | ||||||||
Basic net earnings per common share | 0.80 | 0.28 | 0.76 | 0.61 | ||||||||
Diluted net earnings per common share | 0.78 | 0.27 | 0.75 | 0.60 | ||||||||
93
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None.
| ITEM 9A. | CONTROLS AND PROCEDURES |
EVALUATION OF DISCLOSURE CONTROLS AND PROCEDURES
The Company maintains disclosure controls and procedures as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934 (Exchange Act) that are designed to provide reasonable assurance that information required to be disclosed by the Company in reports that it files or submits under the Exchange Act is (i) recorded, processed, summarized and reported within the time periods specified in SEC rules and forms; and (ii) accumulated and communicated to the Company's management, including its principal executive officer and principal financial officer, as appropriate to allow timely decisions regarding required disclosure.
In connection with the filing of this Form 10-K, management evaluated, under the supervision and with the participation of the Company's Chief Executive Officer and Chief Financial Officer, the effectiveness of the design and operation of the Company's disclosure controls and procedures as of December 31, 2009. Based upon that evaluation, the Company's Chief Executive Officer and Chief Financial Officer concluded that the Company's disclosure controls and procedures were effective at the reasonable assurance level as of December 31, 2009.
CHANGES IN INTERNAL CONTROL OVER FINANCIAL REPORTING
There have been no changes in the Company's internal control over financial reporting during the quarter ended December 31, 2009 that have materially affected, or are reasonably likely to materially affect, the Company's internal control over financial reporting.
94
Report of Management on Internal Control over Financial Reporting as of December 31, 2009
The Company's management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rules 13a-15(f) and 15d-15(f) under the Securities Exchange Act of 1934. The Company's internal control system is designed to provide reasonable assurance to our management and board of directors regarding the reliability of financial reporting and the preparation of consolidated financial statements for external purposes in accordance with generally accepted accounting principles. The Company's internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the Company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of consolidated financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the Company are being made only in accordance with authorizations of management and directors of the Company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the Company's assets that could have a material effect on the consolidated financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Management assessed the effectiveness of the Company's internal control over financial reporting as of December 31, 2009. In making this assessment, we used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control - Integrated Framework . Based on our assessment and those criteria, we believe that, as of December 31, 2009, the Company maintained effective internal control over financial reporting.
The Company's independent registered public accounting firm has audited the Company's internal control over financial reporting as of December 31, 2009, as stated in the Report of Independent Registered Public Accounting Firm, appearing under Item 9A, which expresses an unqualified opinion on the effectiveness of the Company's internal controls over financial reporting as of December 31, 2009.
/s/ STEPHEN J. HEMSLEY |
Stephen J. Hemsley President and Chief Executive Officer |
/s/ GEORGE L. MIKAN III |
George L. Mikan III Executive Vice President and Chief Financial Officer |
/s/ ERIC S. RANGEN |
Eric S. Rangen Senior Vice President and Chief Accounting Officer |
February 10, 2010
95
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders of UnitedHealth Group Incorporated and subsidiaries:
We have audited the internal control over financial reporting of UnitedHealth Group Incorporated and subsidiaries (the "Company") as of December 31, 2009, based on criteria established in Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. The Company's management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Report of Management on Internal Control Over Financial Reporting as of December 31, 2009. Our responsibility is to express an opinion on the Company's internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company's internal control over financial reporting is a process designed by, or under the supervision of, the company's principal executive and principal financial officers, or persons performing similar functions, and effected by the company's board of directors, management, and other personnel to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company's internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company's assets that could have a material effect on the financial statements.
Because of the inherent limitations of internal control over financial reporting, including the possibility of collusion or improper management override of controls, material misstatements due to error or fraud may not be prevented or detected on a timely basis. Also, projections of any evaluation of the effectiveness of the internal control over financial reporting to future periods are subject to the risk that the controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2009, based on the criteria established in Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated financial statements as of and for the year ended December 31, 2009 of the Company and our reports dated February 10, 2010 expressed an unqualified opinion on those consolidated financial statements and financial statement schedule.
| /s/ DELOITTE & TOUCHE LLP |
| Minneapolis, MN |
| February 10, 2010 |
96
| ITEM 9B. | OTHER INFORMATION |
None.
PART III
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
Pursuant to General Instruction G(3) to Form 10-K and Instruction 3 to Item 401(b) of Regulation S-K, information regarding our executive officers is provided in Item 1 of Part I of this Annual Report on Form 10-K under the caption "Executive Officers of the Registrant."
The remaining information required by Items 401, 405, 406 and 407(c)(3), (d)(4) and (d)(5) of Regulation S-K will be included under the headings "Corporate Governance," "Election of Directors" and "Section 16(a) Beneficial Ownership Reporting Compliance" in our definitive proxy statement for our Annual Meeting of Shareholders to be held May 25, 2010, and such required information is incorporated herein by reference.
| ITEM 11. | EXECUTIVE COMPENSATION |
The information required by Items 402, 407(e)(4) and (e)(5) of Regulation S-K will be included under the headings "Executive Compensation" and "Compensation Committee Interlocks and Insider Participation" in our definitive proxy statement for our Annual Meeting of Shareholders to be held May 25, 2010, and such required information is incorporated herein by reference.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
Equity Compensation Plan Information
The following table sets forth certain information, as of December 31, 2009, concerning shares of common stock authorized for issuance under all of our equity compensation plans.
Plan Category | (a) Number of securities to be issued upon exercise of outstanding options, warrants and rights (3) | (b) Weighted-average exercise price of outstanding options, warrants and rights (3) | (c) Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in column (a)) | |||||
Equity compensation plans approved by shareholders (1) | 80,727,176 | $ | 34.61 | 72,777,932 | (4) | |||
Equity compensation plans not approved by shareholders (2) | - | - | - | |||||
Total (2) | 80,727,176 | $ | 34.61 | 72,777,932 | ||||
| (1) | Consists of the UnitedHealth Group Incorporated 2002 Stock Incentive Plan, as amended, and the UnitedHealth Group 1993 Employee Stock Purchase Plan, as amended. Includes 6,170,280 options to acquire shares of common stock that were originally issued under the United HealthCare Corporation 1998 Broad-Based Stock Incentive Plan, as amended, which was not approved by the Company's shareholders, but the shares issuable under the 1998 Broad-Based Stock Incentive Plan were subsequently included in the number of shares approved by the Company's shareholders when approving the 2002 Stock Incentive Plan. |
| (2) | Excludes 950,529 shares underlying stock options assumed by us in connection with our acquisition of the companies under whose plans the options originally were granted. These options have a weighted-average |
97
exercise price of $23.51 and an average remaining term of approximately 2.7 years. The options are administered pursuant to the terms of the plan under which the option originally was granted. No future awards will be granted under these acquired plans. |
| (3) | Excludes SARs to acquire 42,467,803 shares of common stock of the Company with exercise prices above $30.48, the closing price of a share of our common stock as reported on the NYSE on December 31, 2009. |
| (4) | Includes 9,326,472 shares of common stock available for future issuance under the Employee Stock Purchase Plan as of December 31, 2009, and 63,451,460 shares available under the 2002 Stock Incentive Plan as of December 31, 2009. Shares available under the 2002 Stock Incentive Plan may become the subject of future awards in the form of stock options, SARs, restricted stock, restricted stock units, performance awards and other stock-based awards, except that only 15,274,665 of these shares are available for future grants of awards other than stock options or SARs. |
The information required by Item 403 of Regulation S-K will be included under the heading "Security Ownership of Certain Beneficial Owners and Management" in our definitive proxy statement for our Annual Meeting of Shareholders to be held May 25, 2010, and such required information is incorporated herein by reference.
| ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
The information required by Items 404 and 407(a) of Regulation S-K will be included under the headings "Certain Relationships and Transactions" and "Corporate Governance" in our definitive proxy statement for the Annual Meeting of Shareholders to be held May 25, 2010, and such required information is incorporated herein by reference.
| ITEM 14. | PRINCIPAL ACCOUNTANT FEES AND SERVICES |
The information required by Item 9(e) of Schedule 14A will be included under the heading "Independent Registered Public Accounting Firm" in our definitive proxy statement for the Annual Meeting of Shareholders to be held May 25, 2010, and such required information is incorporated herein by reference.
98
PART IV
| ITEM 15. | EXHIBITS AND FINANCIAL STATEMENT SCHEDULES |
| (a) | 1 . Financial Statements |
The financial statements are included under Item 8 of this report:
Consolidated Statements of Operations for the year ended December 31, 2009, 2008 and 2007.
Consolidated Balance Sheets as of December 31, 2009 and 2008.
Consolidated Statements of Changes in Shareholders' Equity for the year ended December 31, 2009, 2008 and 2007.
Consolidated Statements of Cash Flows for the year ended December 31, 2009, 2008 and 2007.
Notes to the Consolidated Financial Statements.
Reports of Independent Registered Public Accounting Firm.
2 . Financial Statement Schedules
The following financial statement schedule of the Company is included in Item 15(c):
Schedule I - Condensed Financial Information of Registrant (Parent Company Only).
All other schedules for which provision is made in the applicable accounting regulations of the SEC are not required under the related instructions, are inapplicable, or the required information is included in the consolidated financial statements, and therefore have been omitted.
3. Exhibits**
| 3.1 | Third Restated Articles of Incorporation of UnitedHealth Group Incorporated (incorporated by reference to Exhibit 3.1 to the Company's Current Report on Form 8-K dated May 29, 2007) | |
| 3.2 | Fourth Amended and Restated Bylaws of UnitedHealth Group Incorporated (incorporated by reference to Exhibit 3.1 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| 4.1 | Senior Indenture, dated as of November 15, 1998, between United HealthCare Corporation and The Bank of New York (incorporated by reference to Exhibit 4.1 to the Company's Registration Statement on Form S-3/A, SEC File Number 333-66013, filed on January 11, 1999) | |
| 4.2 | Amendment, dated as of November 6, 2000, to Senior Indenture, dated as of November 15, 1998, between the UnitedHealth Group Incorporated and The Bank of New York (incorporated by reference to Exhibit 4.1 to the Company's Quarterly Report on Form 10-Q for the quarter ended September 30, 2001) | |
| 4.3 | Instrument of Resignation, Appointment and Acceptance of Trustee, dated January 8, 2007, pursuant to the Senior Indenture, dated November 15, 1988, amended November 6, 2000, among UnitedHealth Group Incorporated, The Bank of New York and Wilmington Trust Company (incorporated by reference to Exhibit 4.3 to the Company's Quarterly Report on Form 10-Q for the quarter ended June 30, 2007) | |
| 4.4 | Indenture, dated as of February 4, 2008, between UnitedHealth Group Incorporated and U.S. Bank National Association (incorporated by reference to Exhibit 4.1 to the Company's Registration Statement on Form S-3, SEC File Number 333-149031, filed on February 4, 2008) | |
99
| *10.1 | UnitedHealth Group Incorporated 2002 Stock Incentive Plan, Amended and Restated Effective May 15, 2002 (incorporated by reference to Exhibit 10(a) to the Company's Annual Report on Form 10-K for the year ended December 31, 2002) | |
| *10.2 | Amendment to the UnitedHealth Group Incorporated 2002 Stock Incentive Plan (incorporated by reference to Exhibit 10.2 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.3 | Form of Agreement for Initial Stock Option Award to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on April 17, 2007 (incorporated by reference to Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2007) | |
| *10.4 | Form of Agreement for Stock Option Award to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on October 31, 2006 (incorporated by reference to Exhibit 10(d) to the Company's Annual Report on Form 10-K for the year ended December 31, 2006) | |
| *10.5 | Form of Agreement for Initial Restricted Stock Unit Award to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on April 17, 2007 (incorporated by reference to Exhibit 10.2 to the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2007) | |
| *10.6 | Form of Stock Appreciation Rights Award Agreement to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on October 31, 2006 (incorporated by reference to Exhibit 10(e) to the Company's Annual Report on Form 10-K for the year ended December 31, 2006) | |
| *10.7 | Form of Agreement for Stock Option Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.1 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.8 | Form of Agreement for Restricted Stock Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.2 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.9 | Form of Agreement for Restricted Stock Unit Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.3 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.10 | Form of Agreement for Stock Appreciation Rights Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.4 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.11 | Form of Agreement for Performance-based Restricted Stock Unit Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.5 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.12 | Amended and Restated UnitedHealth Group Incorporated Executive Incentive Plan (2009 Statement), effective as of December 31, 2008 (incorporated by reference to Exhibit 10.12 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.13 | Amended and Restated UnitedHealth Group Incorporated 2008 Executive Incentive Plan, effective as of December 31, 2008 (incorporated by reference to Exhibit 10.13 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.14 | UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10(e) of the Company's Annual Report on Form 10-K for the year ended December 31, 2003) | |
| *10.15 | First Amendment to UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10.3 to the Company's Current Report on Form 8-K dated October 31, 2006) | |
100
| *10.16 | Second Amendment to UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10.13 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.17 | Third Amendment to UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10.17 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.18 | Summary of Non-Management Director Compensation, effective as of July 1, 2009 (incorporated by reference to Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the quarter ended June 30, 2009) | |
| *10.19 | UnitedHealth Group Directors' Compensation Deferral Plan (2009 Statement) (incorporated by reference to Exhibit 10.18 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.20 | Amendment to the UnitedHealth Group Directors' Compensation Deferral Plan, effective as of January 1, 2010 | |
| *10.21 | Employment Agreement, dated as of November 7, 2006, between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit 10.1 to the Company's Current Report on Form 8-K dated November 7, 2006) | |
| *10.22 | Agreement for Supplemental Executive Retirement Pay, effective April 1, 2004, between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit 10(b) to the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2004) | |
| *10.23 | Amendment to Agreement for Supplemental Executive Retirement Pay, dated as of November 7, 2006, between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit A to Exhibit 10.1 to the Company's Current Report on Form 8-K dated November 7, 2006) | |
| *10.24 | Amendment to Employment Agreement and Agreement for Supplemental Executive Retirement Pay, effective as of December 31, 2008, between United HealthCare Services, Inc. and Stephen J. Hemsley (incorporated by reference to Exhibit 10.22 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.25 | Letter Agreement, effective as of February 19, 2008, by and between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit 10.22 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.26 | Employment Agreement, effective as of November 7, 2006, by and between United HealthCare Services, Inc. and George L. Mikan III (incorporated by reference to Exhibit 10.1 to the Company's Current Report on Form 8-K dated January 30, 2007) | |
| *10.27 | Amendment to Employment Agreement, effective as of December 31, 2008, between United HealthCare Services, Inc. and George L. Mikan III (incorporated by reference to Exhibit 10.25 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.28 | Employment Agreement, dated as of April 10, 2007, between United HealthCare Services, Inc. and William A. Munsell (incorporated by reference to Exhibit 10.24 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.29 | Amendment to Employment Agreement, effective as of December 31, 2008, between United HealthCare Services, Inc. and William A. Munsell (incorporated by reference to Exhibit 10.27 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.30 | Employment Agreement, effective as of April 12, 2007, between United HealthCare Services, Inc. and Anthony Welters (incorporated by reference to Exhibit 10.28 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
101
| *10.31 | Amendment to Employment Agreement, effective as of December 31, 2008, between United HealthCare Services, Inc. and Anthony Welters (incorporated by reference to Exhibit 10.35 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.32 | Employment Agreement, effective as of January 29, 2009, between United HealthCare Services, Inc. and Larry C. Renfro (incorporated by reference to Exhibit 10.40 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| 11.1 | Statement regarding computation of per share earnings (incorporated by reference to the information contained under the heading "Net Earnings Per Common Share" in Note 2 to the Notes to Consolidated Financial Statements included under Item 8) | |
| 12.1 | Ratio of Earnings to Fixed Charges | |
| 21.1 | Subsidiaries of the Company | |
| 23.1 | Consent of Independent Registered Public Accounting Firm | |
| 24.1 | Power of Attorney | |
| 31.1 | Certifications pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 32.1 | Certifications pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |
| 101 | The following materials from UnitedHealth Group Incorporated's Annual Report on Form 10-K for the year ended December 31, 2009, filed on February 10, 2010, formatted in XBRL (eXtensible Business Reporting Language): (i) Consolidated Balance Sheets, (ii) Consolidated Statements of Operations, (iii) Consolidated Statements of Changes in Shareholders' Equity, (iv) Consolidated Statements of Cash Flows, and (v) Notes to the Consolidated Financial Statements, tagged as blocks of text. | |
| * | Denotes management contracts and compensation plans in which certain directors and named executive officers participate and which are being filed pursuant to Item 601(b)(10)(iii)(A) of Regulation S-K. |
| ** | Pursuant to Item 601(b)(4)(iii) of Regulation S-K, copies of instruments defining the rights of certain holders of long-term debt are not filed. The Company will furnish copies thereof to the SEC upon request(c) Financial Statement Schedule |
| (c) | Financial Statement Schedule |
Schedule I - Condensed Financial Information of Registrant (Parent Company Only).
102
Schedule I
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Shareholders of UnitedHealth Group Incorporated and subsidiaries:
We have audited the consolidated financial statements of UnitedHealth Group Incorporated and subsidiaries (the "Company") as of December 31, 2009 and 2008, and for each of the three years in the period ended December 31, 2009, and the Company's internal control over financial reporting as of December 31, 2009, and have issued our reports thereon dated February 10, 2010; such consolidated financial statements and reports are included in your 2009 Annual Report to Stockholders and are incorporated herein by reference. Our audits also included the consolidated financial statement schedule of the Company listed in Item 15. This consolidated financial statement schedule is the responsibility of the Company's management. Our responsibility is to express an opinion based on our audits. In our opinion, the consolidated financial statement schedule, when considered in relation to the basic consolidated financial statements taken as a whole, present fairly, in all material respects, the information set forth therein.
| /s/ DELOITTE & TOUCHE LLP |
| Minneapolis, MN |
| February 10, 2010 |
103
Schedule I
Condensed Financial Information of Registrant
(Parent Company Only)
UnitedHealth Group
Condensed Balance Sheets
| December 31, | ||||||||
(in millions, except per share data) | 2009 | 2008 | ||||||
ASSETS | ||||||||
Current assets: | ||||||||
Cash and cash equivalents | $ | 2,309 | $ | 880 | ||||
Deferred income taxes | 163 | 169 | ||||||
Prepaid expenses and other current assets | 61 | 196 | ||||||
Total current assets | 2,533 | 1,245 | ||||||
Equity in net assets of subsidiaries | 32,812 | 32,636 | ||||||
Other assets | 60 | 685 | ||||||
TOTAL ASSETS | $ | 35,405 | $ | 34,566 | ||||
LIABILITIES AND SHAREHOLDERS' EQUITY | ||||||||
Current liabilities: | ||||||||
Accounts payable and accrued liabilities | $ | 522 | $ | 805 | ||||
Note payable to subsidiary | 100 | 100 | ||||||
Commercial paper and current maturities of long-term debt | 2,164 | 1,456 | ||||||
Total current liabilities | 2,786 | 2,361 | ||||||
Long-term debt, less current maturities | 9,009 | 11,338 | ||||||
Deferred income taxes and other liabilities | 4 | 87 | ||||||
Total liabilities | 11,799 | 13,786 | ||||||
Commitments and contingencies (Note 3) | ||||||||
Shareholders' equity: | ||||||||
Preferred stock, $0.001 par value - 10 shares authorized; no shares issued or outstanding | - | - | ||||||
Common stock, $0.01 par value - 3,000 shares authorized; 1,147 and 1,201 issued and outstanding | 11 | 12 | ||||||
Additional paid-in capital | - | 38 | ||||||
Retained earnings | 23,342 | 20,782 | ||||||
Accumulated other comprehensive (loss) income: | ||||||||
Net unrealized gains (losses) on investments, net of tax effects | 277 | (30 | ) | |||||
Foreign currency translation loss | (24 | ) | (22 | ) | ||||
Total shareholders' equity | 23,606 | 20,780 | ||||||
TOTAL LIABILITIES AND SHAREHOLDERS' EQUITY | $ | 35,405 | $ | 34,566 | ||||
See Notes to the Condensed Financial Statements of Registrant.
104
Schedule I
Condensed Financial Information of Registrant
(Parent Company Only)
UnitedHealth Group
Condensed Statements of Operations
| For the Year Ended December 31, | ||||||||||||
(in millions) | 2009 | 2008 | 2007 | |||||||||
REVENUES: | ||||||||||||
Investment and other income | $ | 10 | $ | 20 | $ | 78 | ||||||
Total revenues | 10 | 20 | 78 | |||||||||
OPERATING COSTS: | ||||||||||||
Operating costs | 5 | 1,256 | 57 | |||||||||
Interest expense | 509 | 565 | 458 | |||||||||
Total operating costs | 514 | 1,821 | 515 | |||||||||
LOSS BEFORE INCOME TAXES | (504 | ) | (1,801 | ) | (437 | ) | ||||||
Benefit for income taxes | 172 | 641 | 159 | |||||||||
LOSS OF PARENT COMPANY | (332 | ) | (1,160 | ) | (278 | ) | ||||||
Equity in undistributed income of subsidiaries | 4,154 | 4,137 | 4,932 | |||||||||
NET EARNINGS | $ | 3,822 | $ | 2,977 | $ | 4,654 | ||||||
See Notes to the Condensed Financial Statements of Registrant.
105
Schedule I
Condensed Financial Information of Registrant
(Parent Company Only)
UnitedHealth Group
Condensed Statements of Cash Flows
| For the Year Ended December 31, | ||||||||||||
(in millions) | 2009 | 2008 | 2007 | |||||||||
OPERATING ACTIVITIES | ||||||||||||
Cash flows from operating activities | $ | 5,065 | $ | 3,962 | $ | 4,178 | ||||||
INVESTING ACTIVITIES | ||||||||||||
Capital contributions to subsidiaries | (90 | ) | (7 | ) | (1,272 | ) | ||||||
Cash paid for acquisitions | (1,045 | ) | (4,419 | ) | (270 | ) | ||||||
Cash received from dispositions | - | 185 | - | |||||||||
Cash flows used for investing activities | (1,135 | ) | (4,241 | ) | (1,542 | ) | ||||||
FINANCING ACTIVITIES | ||||||||||||
(Repayments of) proceeds from commercial paper, net | (99 | ) | (1,346 | ) | 947 | |||||||
Proceeds from issuance of long-term debt | - | 2,981 | 3,582 | |||||||||
Payments for retirement of long-term debt | (1,350 | ) | (500 | ) | (950 | ) | ||||||
Proceeds from interest rate swap termination | 513 | - | - | |||||||||
Repayment of note to subsidiary | - | - | (60 | ) | ||||||||
Proceeds from issuance of note to subsidiary | - | 100 | - | |||||||||
Common stock repurchases | (1,801 | ) | (2,684 | ) | (6,599 | ) | ||||||
Proceeds from common stock issuances | 282 | 299 | 712 | |||||||||
Share-based compensation excess tax benefits | 38 | 62 | 303 | |||||||||
Dividends paid | (36 | ) | (37 | ) | (40 | ) | ||||||
Other | (48 | ) | (143 | ) | (30 | ) | ||||||
Cash flows used for financing activities | (2,501 | ) | (1,268 | ) | (2,135 | ) | ||||||
INCREASE (DECREASE) IN CASH AND CASH EQUIVALENTS | 1,429 | (1,547 | ) | 501 | ||||||||
CASH AND CASH EQUIVALENTS, BEGINNING OF PERIOD | 880 | 2,427 | 1,926 | |||||||||
CASH AND CASH EQUIVALENTS, END OF PERIOD | $ | 2,309 | $ | 880 | $ | 2,427 | ||||||
Supplemental cash flow disclosures | ||||||||||||
Cash paid for interest | $ | 485 | $ | 547 | $ | 469 | ||||||
Cash paid for income taxes | $ | 2,048 | $ | 1,882 | $ | 2,277 | ||||||
See Notes to the Condensed Financial Statements of Registrant.
106
Schedule I
Condensed Financial Information of Registrant
(Parent Company Only)
UnitedHealth Group
Notes to Condensed Financial Statements
For the Years Ended December 31, 2009, 2008 and 2007
1. Basis of Presentation
UnitedHealth Group's parent company financial information has been derived from its consolidated financial statements and should be read in conjunction with the consolidated financial statements included in this Form 10-K. The accounting policies for the registrant are the same as those described in the Summary of Significant Accounting Policies in Note 2 of Notes to the Consolidated Financial Statements.
2. Subsidiary Transactions
Investment in Subsidiaries. UnitedHealth Group's investment in subsidiaries is stated at cost plus equity in undistributed earnings of subsidiaries.
Dividends. Cash dividends received from subsidiaries and included in Cash Flows from Operating Activities in the Condensed Statements of Cash Flows were $5.4 billion, $1.8 billion and $3.8 billion in 2009, 2008 and 2007, respectively.
3. Commercial Paper and Long-Term Debt
Further discussion of maturities of commercial paper and long-term debt can be found in Note 9 of Notes to the Consolidated Financial Statements.
4. Commitments and Contingencies
Operating costs for 2008 included $350 million for the settlement of class action litigation related to reimbursement for out-of-network medical services. For detail on the proposed settlement and other commitments and contingencies, see Note 14 of Notes to the Consolidated Financial Statements.
5. Acquisitions
See Note 3 of Notes to the Consolidated Financial Statements for a description of acquisitions.
107
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
Dated: February 10, 2010
| UNITEDHEALTH GROUP INCORPORATED | ||
| By | / S / STEPHEN J. HEMSLEY | |
Stephen J. Hemsley President and Chief Executive Officer | ||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Signature | Title | Date | ||
/S/ STEPHEN J. HEMSLEY Stephen J. Hemsley | Director, President and Chief Executive Officer (principal executive officer) | February 10, 2010 | ||
/S/ GEORGE L. MIKAN III George L. Mikan III | Executive Vice President and Chief Financial Officer (principal financial officer) | February 10, 2010 | ||
/S/ ERIC S. RANGEN Eric S. Rangen | Senior Vice President and Chief Accounting Officer (principal accounting officer) | February 10, 2010 | ||
* William C. Ballard, Jr. | Director | February 10, 2010 | ||
* Richard T. Burke | Director | February 10, 2010 | ||
* Robert J. Darretta | Director | February 10, 2010 | ||
* Michele J. Hooper | Director | February 10, 2010 | ||
* Douglas W. Leatherdale | Director | February 10, 2010 | ||
* Glenn M. Renwick | Director | February 10, 2010 | ||
Kenneth I. Shine | Director | February 10, 2010 | ||
* Gail R. Wilensky | Director | February 10, 2010 | ||
| *By | / S / CHRISTOPHER J. WALSH | |
Christopher J. Walsh, As Attorney-in-Fact |
108
EXHIBIT INDEX **
| 3.1 | Third Restated Articles of Incorporation of UnitedHealth Group Incorporated (incorporated by reference to Exhibit 3.1 to the Company's Current Report on Form 8-K dated May 29, 2007) | |
| 3.2 | Fourth Amended and Restated Bylaws of UnitedHealth Group Incorporated (incorporated by reference to Exhibit 3.1 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| 4.1 | Senior Indenture, dated as of November 15, 1998, between United HealthCare Corporation and The Bank of New York (incorporated by reference to Exhibit 4.1 to the Company's Registration Statement on Form S-3/A, SEC File Number 333-66013, filed on January 11, 1999) | |
| 4.2 | Amendment, dated as of November 6, 2000, to Senior Indenture, dated as of November 15, 1998, between the UnitedHealth Group Incorporated and The Bank of New York (incorporated by reference to Exhibit 4.1 to the Company's Quarterly Report on Form 10-Q for the quarter ended September 30, 2001) | |
| 4.3 | Instrument of Resignation, Appointment and Acceptance of Trustee, dated January 8, 2007, pursuant to the Senior Indenture, dated November 15, 1988, amended November 6, 2000, among UnitedHealth Group Incorporated, The Bank of New York and Wilmington Trust Company (incorporated by reference to Exhibit 4.3 to the Company's Quarterly Report on Form 10-Q for the quarter ended June 30, 2007) | |
| 4.4 | Indenture, dated as of February 4, 2008, between UnitedHealth Group Incorporated and U.S. Bank National Association (incorporated by reference to Exhibit 4.1 to the Company's Registration Statement on Form S-3, SEC File Number 333-149031, filed on February 4, 2008) | |
| *10.1 | UnitedHealth Group Incorporated 2002 Stock Incentive Plan, Amended and Restated Effective May 15, 2002 (incorporated by reference to Exhibit 10(a) to the Company's Annual Report on Form 10-K for the year ended December 31, 2002) | |
| *10.2 | Amendment to the UnitedHealth Group Incorporated 2002 Stock Incentive Plan (incorporated by reference to Exhibit 10.2 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.3 | Form of Agreement for Initial Stock Option Award to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on April 17, 2007 (incorporated by reference to Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2007) | |
| *10.4 | Form of Agreement for Stock Option Award to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on October 31, 2006 (incorporated by reference to Exhibit 10(d) to the Company's Annual Report on Form 10-K for the year ended December 31, 2006) | |
| *10.5 | Form of Agreement for Initial Restricted Stock Unit Award to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on April 17, 2007 (incorporated by reference to Exhibit 10.2 to the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2007) | |
| *10.6 | Form of Stock Appreciation Rights Award Agreement to Non-Employee Directors under the Company's 2002 Stock Incentive Plan, as amended on October 31, 2006 (incorporated by reference to Exhibit 10(e) to the Company's Annual Report on Form 10-K for the year ended December 31, 2006) | |
| *10.7 | Form of Agreement for Stock Option Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.1 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.8 | Form of Agreement for Restricted Stock Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.2 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
109
| *10.9 | Form of Agreement for Restricted Stock Unit Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.3 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.10 | Form of Agreement for Stock Appreciation Rights Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.4 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.11 | Form of Agreement for Performance-based Restricted Stock Unit Award to Executives under the Company's 2002 Stock Incentive Plan, effective as of October 23, 2009 (incorporated by reference to Exhibit 10.5 to the Company's Current Report on Form 8-K dated October 23, 2009) | |
| *10.12 | Amended and Restated UnitedHealth Group Incorporated Executive Incentive Plan (2009 Statement), effective as of December 31, 2008 (incorporated by reference to Exhibit 10.12 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.13 | Amended and Restated UnitedHealth Group Incorporated 2008 Executive Incentive Plan, effective as of December 31, 2008 (incorporated by reference to Exhibit 10.13 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.14 | UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10(e) of the Company's Annual Report on Form 10-K for the year ended December 31, 2003) | |
| *10.15 | First Amendment to UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10.3 to the Company's Current Report on Form 8-K dated October 31, 2006) | |
| *10.16 | Second Amendment to UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10.13 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.17 | Third Amendment to UnitedHealth Group Executive Savings Plan (2004 Statement) (incorporated by reference to Exhibit 10.17 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.18 | Summary of Non-Management Director Compensation, effective as of July 1, 2009 (incorporated by reference to Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the quarter ended June 30, 2009) | |
| *10.19 | UnitedHealth Group Directors' Compensation Deferral Plan (2009 Statement) (incorporated by reference to Exhibit 10.18 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.20 | Amendment to the UnitedHealth Group Directors' Compensation Deferral Plan, effective as of January 1, 2010 | |
| *10.21 | Employment Agreement, dated as of November 7, 2006, between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit 10.1 to the Company's Current Report on Form 8-K dated November 7, 2006) | |
| *10.22 | Agreement for Supplemental Executive Retirement Pay, effective April 1, 2004, between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit 10(b) to the Company's Quarterly Report on Form 10-Q for the quarter ended March 31, 2004) | |
| *10.23 | Amendment to Agreement for Supplemental Executive Retirement Pay, dated as of November 7, 2006, between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit A to Exhibit 10.1 to the Company's Current Report on Form 8-K dated November 7, 2006) | |
110
| *10.24 | Amendment to Employment Agreement and Agreement for Supplemental Executive Retirement Pay, effective as of December 31, 2008, between United HealthCare Services, Inc. and Stephen J. Hemsley (incorporated by reference to Exhibit 10.22 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.25 | Letter Agreement, effective as of February 19, 2008, by and between UnitedHealth Group Incorporated and Stephen J. Hemsley (incorporated by reference to Exhibit 10.22 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.26 | Employment Agreement, effective as of November 7, 2006, by and between United HealthCare Services, Inc. and George L. Mikan III (incorporated by reference to Exhibit 10.1 to the Company's Current Report on Form 8-K dated January 30, 2007) | |
| *10.27 | Amendment to Employment Agreement, effective as of December 31, 2008, between United HealthCare Services, Inc. and George L. Mikan III (incorporated by reference to Exhibit 10.25 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.28 | Employment Agreement, dated as of April 10, 2007, between United HealthCare Services, Inc. and William A. Munsell (incorporated by reference to Exhibit 10.24 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.29 | Amendment to Employment Agreement, effective as of December 31, 2008, between United HealthCare Services, Inc. and William A. Munsell (incorporated by reference to Exhibit 10.27 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.30 | Employment Agreement, effective as of April 12, 2007, between United HealthCare Services, Inc. and Anthony Welters (incorporated by reference to Exhibit 10.28 to the Company's Annual Report on Form 10-K for the year ended December 31, 2007) | |
| *10.31 | Amendment to Employment Agreement, effective as of December 31, 2008, between United HealthCare Services, Inc. and Anthony Welters (incorporated by reference to Exhibit 10.35 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| *10.32 | Employment Agreement, effective as of January 29, 2009, between United HealthCare Services, Inc. and Larry C. Renfro (incorporated by reference to Exhibit 10.40 to the Company's Annual Report on Form 10-K for the year ended December 31, 2008) | |
| 11.1 | Statement regarding computation of per share earnings (incorporated by reference to the information contained under the heading "Net Earnings Per Common Share" in Note 2 to the Notes to Consolidated Financial Statements included under Item 8) | |
| 12.1 | Ratio of Earnings to Fixed Charges | |
| 21.1 | Subsidiaries of the Company | |
| 23.1 | Consent of Independent Registered Public Accounting Firm | |
| 24.1 | Power of Attorney | |
| 31.1 | Certifications pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 32.1 | Certifications pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |
| 101 | The following materials from UnitedHealth Group Incorporated's Annual Report on Form 10-K for the year ended December 31, 2009, filed on February 10, 2010, formatted in XBRL (eXtensible Business Reporting Language): (i) Consolidated Balance Sheets, (ii) Consolidated Statements of Operations, (iii) Consolidated Statements of Changes in Shareholders' Equity, (iv) Consolidated Statements of Cash Flows, and (v) Notes to the Consolidated Financial Statements, tagged as blocks of text. | |
111
| * | Denotes management contracts and compensation plans in which certain directors and named executive officers participate and which are being filed pursuant to Item 601(b)(10)(iii)(A) of Regulation S-K. |
| ** | Pursuant to Item 601(b)(4)(iii) of Regulation S-K, copies of instruments defining the rights of certain holders of long-term debt are not filed. The Company will furnish copies thereof to the SEC upon request(c) Financial Statement Schedule |
112